

Optimal timing of revascularization for patients with non-ST segment elevation myocardial infarction and severe left ventricular dysfunction
- PMID: 39213207
- PMCID: PMC11365634
- DOI: 10.1097/MD.0000000000038483
Optimal timing of revascularization for patients with non-ST segment elevation myocardial infarction and severe left ventricular dysfunction
Abstract
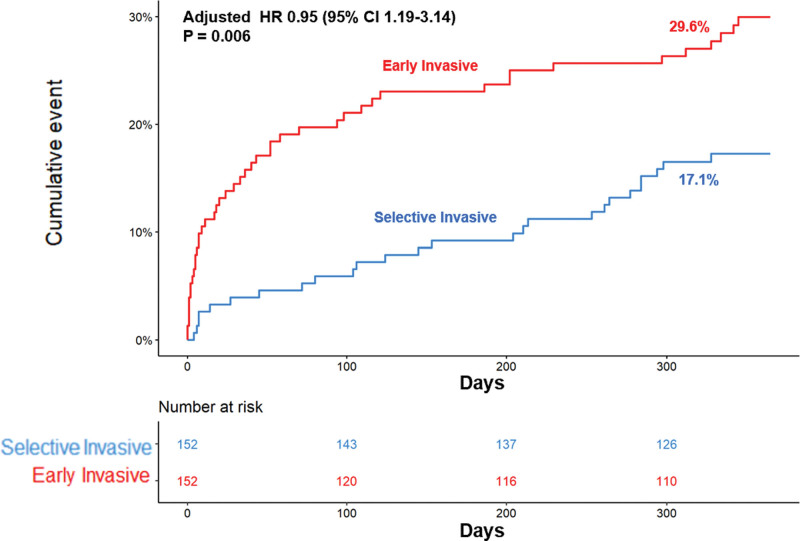
Optimal timing of revascularization for patients who presented with non-ST segment elevation myocardial infarction (NSTEMI) and severe left ventricular (LV) dysfunction is unclear. A total of 386 NSTEMI patients with severe LV dysfunction from the nationwide, multicenter, and prospective Korea Acute Myocardial Infarction Registry V (KAMIR-V) were enrolled. Severe LV dysfunction was defined as LV ejection fraction ≤ 35%. Patients with cardiogenic shock were excluded. Patients were stratified into two groups: PCI within 24 hours (early invasive group) and PCI over 24 hours (selective invasive group). Primary endpoint was major adverse cardiac and cerebrovascular events (MACCE) including all-cause death, non-fatal MI, repeat revascularization, and stroke at 12 months after index procedure. Early invasive group showed higher incidence of in-hospital death (9.4% vs 3.3%, P = .036) and cardiogenic shock (11.5% vs 4.6%, P = .030) after PCI. Early invasive group also showed higher maximum troponin I level during admission (27.7 ± 44.8 ng/mL vs 14.9 ± 24.6 ng/mL, P = .001), compared with the selective invasive group. Early invasive group had an increased risk of 12-month MACCE, compared with selective invasive group (25.6% vs 17.1%; adjusted HR = 2.10, 95% CI 1.17-3.77, P = .006). Among NSTEMI patients with severe LV dysfunction, the early invasive strategy did not improve the clinical outcomes. This data supports that an individualized approach may benefit high-risk NSTEMI patients rather than a routine invasive approach.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures



References
-
- Puymirat E, Simon T, Cayla G, et al.; USIK, USIC 2000, and FAST-MI investigators. Acute myocardial infarction: changes in patient characteristics, management, and 6-month outcomes over a period of 20 years in the FAST-MI program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation. 2017;136:1908–19. - PubMed
-
- Fuster V, Badimon L, Badimon JJ, Chesebro JH. The pathogenesis of coronary artery disease and the acute coronary syndromes (2). N Engl J Med. 1992;326:310–8. - PubMed
-
- Mehta SR, Granger CB, Boden WE, et al.; TIMACS Investigators. Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med. 2009;360:2165–75. - PubMed
-
- Montalescot G, Cayla G, Collet JP, et al.; ABOARD Investigators. Immediate vs delayed intervention for acute coronary syndromes: a randomized clinical trial. JAMA. 2009;302:947–54. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
