

Circulating miRNA panels as a novel non-invasive diagnostic, prognostic, and potential predictive biomarkers in non-small cell lung cancer (NSCLC)
- PMID: 39215192
- PMCID: PMC11473829
- DOI: 10.1038/s41416-024-02831-3
Circulating miRNA panels as a novel non-invasive diagnostic, prognostic, and potential predictive biomarkers in non-small cell lung cancer (NSCLC)
Abstract
Background: Non-small cell lung cancer (NSCLC) is characterised by its aggressiveness and poor prognosis. Early detection and accurate prediction of therapeutic responses remain critical for improving patient outcomes. In the present study, we investigated the potential of circulating microRNA (miRNA) as non-invasive biomarkers in patients with NSCLC.
Methods: We quantified miRNA expression in plasma from 122 participants (78 NSCLC; 44 healthy controls). Bioinformatic tools were employed to identify miRNA panels for accurate NSCLC diagnosis. Validation was performed using an independent publicly available dataset of more than 4000 NSCLC patients. Next, we correlated miRNA expression with clinicopathological information to identify independent prognostic miRNAs and those predictive of anti-PD-1 treatment response.
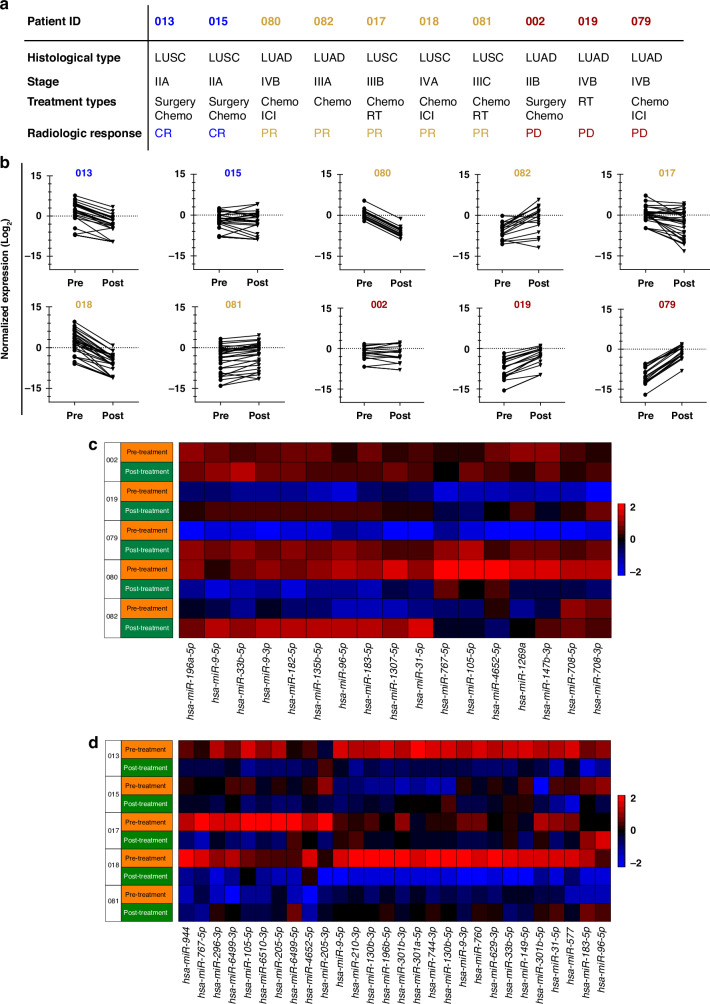
Results: We identified miRNA panels for lung adenocarcinoma (LUAD) and squamous cell carcinoma (LUSC) diagnosis. The LUAD panel consists of seven circulating miRNAs (miR-9-3p, miR-96-5p, miR-147b-3p, miR-196a-5p, miR-708-3p, miR-708-5p, miR-4652-5p), while the LUSC panel comprises nine miRNAs (miR-130b-3p, miR-269-3p, miR-301a-5p, miR-301b-5p, miR-744-3p, miR-760, miR-767-5p, miR-4652-5p, miR-6499-3p). Additionally, miR-135b-5p, miR-196a-5p, miR-31-5p (LUAD), and miR-205 (LUSC) serve as independent prognostic markers for survival. Furthermore, two miRNA clusters, namely miR-183/96/182 and miR-767/105, exhibit predictive potential in anti-PD-1-treated LUAD patients.
Conclusions: Circulating miRNA signatures demonstrate diagnostic and prognostic value for NSCLC and may guide treatment decisions in clinical practice.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
