

Electrolyte disorders related emergencies in children
- PMID: 39215244
- PMCID: PMC11363364
- DOI: 10.1186/s12882-024-03725-5
Electrolyte disorders related emergencies in children
Abstract
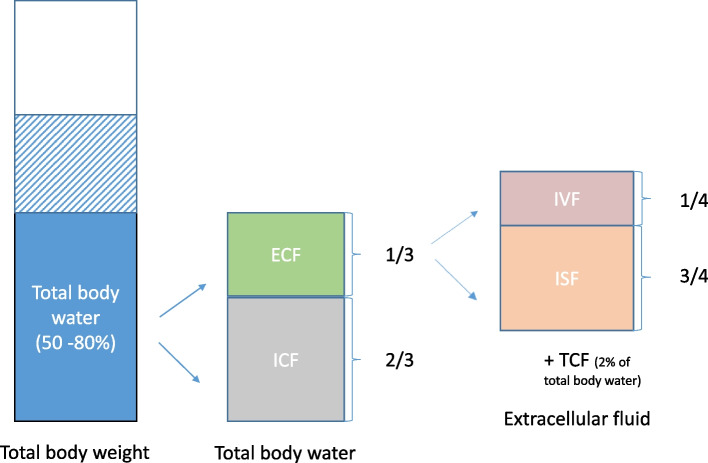
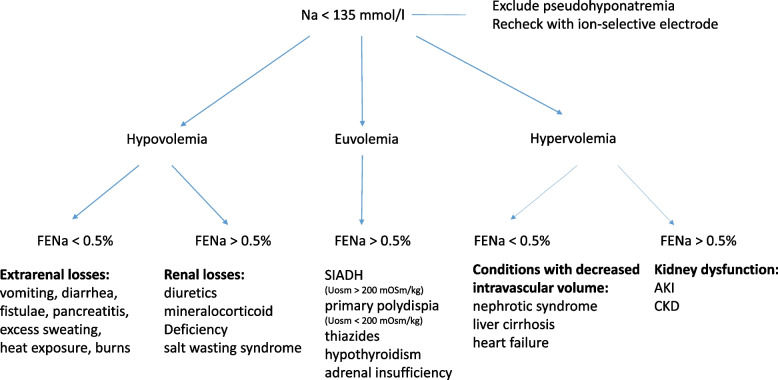
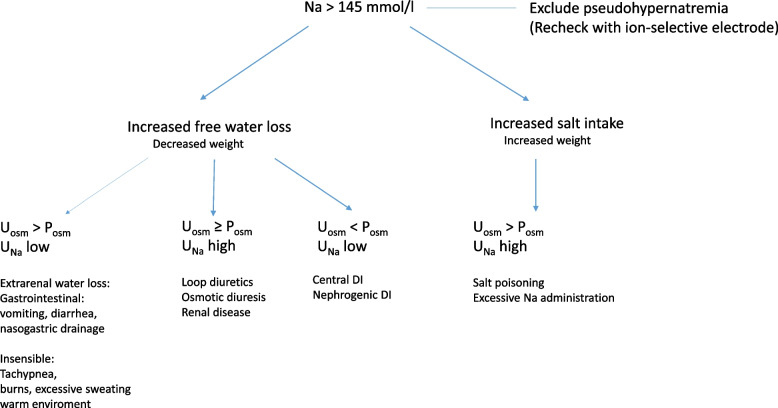
This article provides a comprehensive overview of electrolyte and water homeostasis in pediatric patients, focusing on some of the common serum electrolyte abnormalities encountered in clinical practice. Understanding pathophysiology, taking a detailed history, performing comprehensive physical examinations, and ordering basic laboratory investigations are essential for the timely proper management of these conditions. We will discuss the pathophysiology, clinical manifestations, diagnostic approaches, and treatment strategies for each electrolyte disorder. This article aims to enhance the clinical approach to pediatric patients with electrolyte imbalance-related emergencies, ultimately improving patient outcomes.Trial registration This manuscript does not include a clinical trial; instead, it provides an updated review of literature.
Keywords: Electrolyte imbalances; Hypercalcemia; Hyperkalemia; Hypernatremia; Hypocalcemia; Hypokalemia; Hyponatremia; Pediatrics.
© 2024. The Author(s).
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
