

Septic shock in the immunocompromised cancer patient: a narrative review
- PMID: 39215292
- PMCID: PMC11363658
- DOI: 10.1186/s13054-024-05073-0
Septic shock in the immunocompromised cancer patient: a narrative review
Abstract
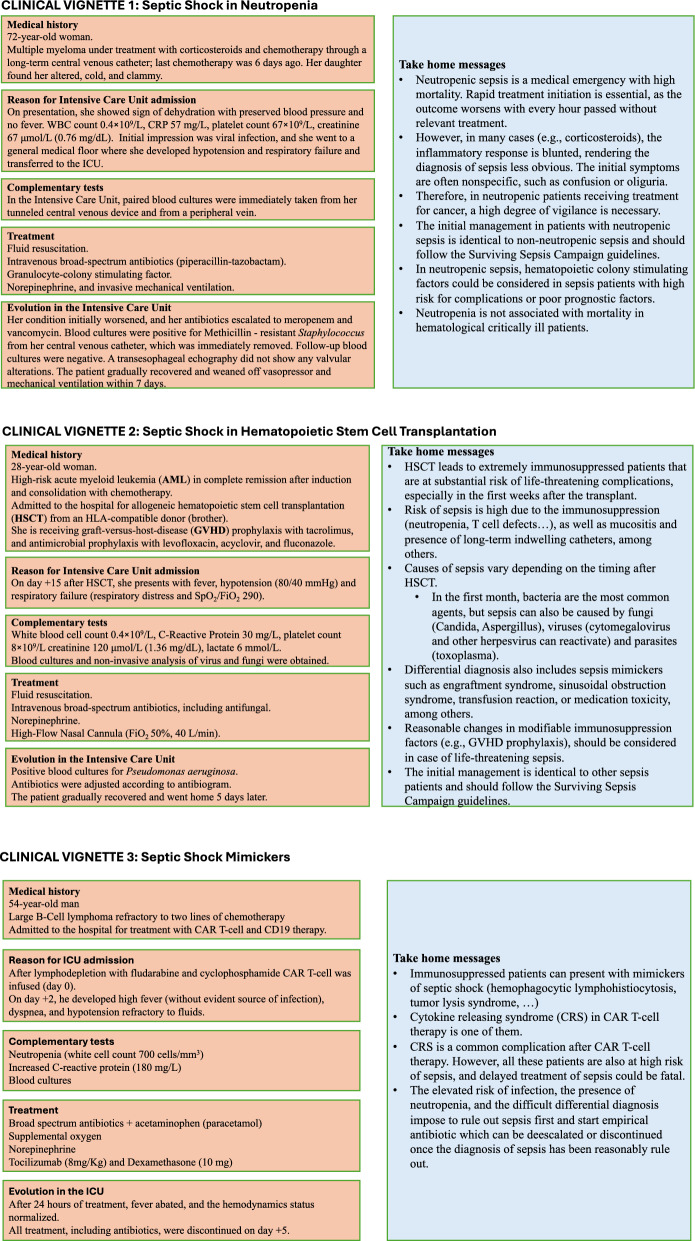
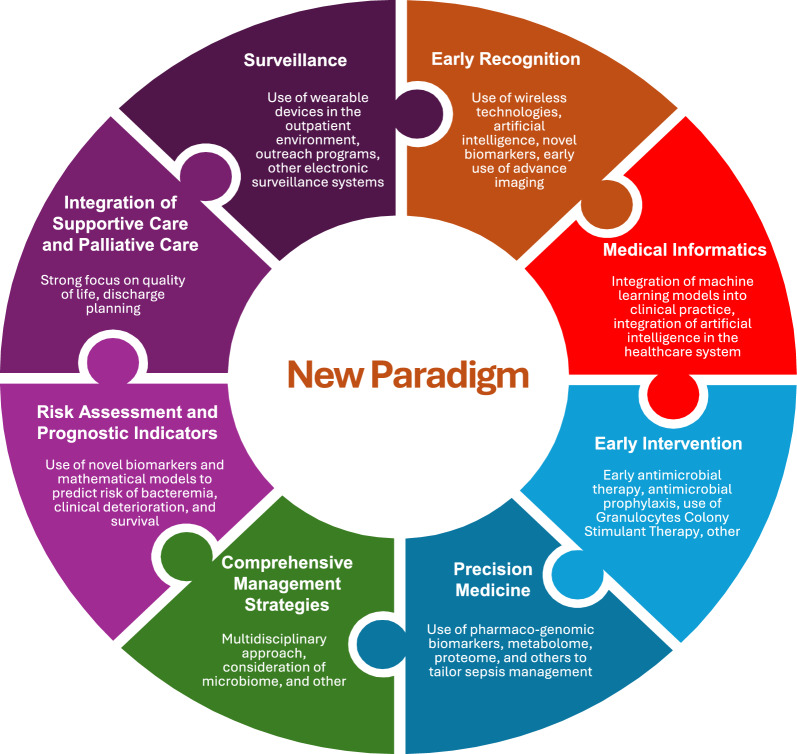
Immunosuppressed patients, particularly those with cancer, represent a momentous and increasing portion of the population, especially as cancer incidence rises with population growth and aging. These patients are at a heightened risk of developing severe infections, including sepsis and septic shock, due to multiple immunologic defects such as neutropenia, lymphopenia, and T and B-cell impairment. The diverse and complex nature of these immunologic profiles, compounded by the concomitant use of immunosuppressive therapies (e.g., corticosteroids, cytotoxic drugs, and immunotherapy), superimposed by the breakage of natural protective barriers (e.g., mucosal damage, chronic indwelling catheters, and alterations of anatomical structures), increases the risk of various infections. These and other conditions that mimic sepsis pose substantial diagnostic and therapeutic challenges. Factors that elevate the risk of progression to septic shock in these patients include advanced age, pre-existing comorbidities, frailty, type of cancer, the severity of immunosuppression, hypoalbuminemia, hypophosphatemia, Gram-negative bacteremia, and type and timing of responses to initial treatment. The management of vulnerable cancer patients with sepsis or septic shock varies due to biased clinical practices that may result in delayed access to intensive care and worse outcomes. While septic shock is typically associated with poor outcomes in patients with malignancies, survival has significantly improved over time. Therefore, understanding and addressing the unique needs of cancer patients through a new paradigm, which includes the integration of innovative technologies into our healthcare system (e.g., wireless technologies, medical informatics, precision medicine), targeted management strategies, and robust clinical practices, including early identification and diagnosis, coupled with prompt admission to high-level care facilities that promote a multidisciplinary approach, is crucial for improving their prognosis and overall survival rates.
Keywords: Critical care; Critical care outcomes; Hematologic neoplasms; Hematopoietic stem cell transplantation; Immunocompromised host; Neoplasms; Organ transplantation; Septic shock.
© 2024. The Author(s).
Conflict of interest statement
FP received lecture and consulting fees from Gilead. PC received honoraria for scientific collaboration from Pfizer, MSD, Gilead, and AbbVie, and advisory board fees from Alexion, Janssen, Sanofi and Gilead. PP received lecture fees from Gilead, Pfizer, Mundipharma, MSD and advisory board fees from Biocodex, Gilead. SD received lecture fees from Octapharm, OrphaSwiss, Alexion and advisory board fees from Alexion, Santersus, and Pantherna. The other authors declare no conflict of interest applicable to this work.
Figures
References
-
- Guidelines for intensive care unit admission discharge and triage. Task force of the American college of critical care medicine society of critical care medicine. Crit Care Med. 1999;27:633–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
