

Safety and Efficacy of Bimekizumab in Patients with Psoriatic Arthritis: 2-Year Results from Two Phase 3 Studies
- PMID: 39215949
- PMCID: PMC11422409
- DOI: 10.1007/s40744-024-00708-8
Safety and Efficacy of Bimekizumab in Patients with Psoriatic Arthritis: 2-Year Results from Two Phase 3 Studies
Erratum in
-
Correction: Safety and Efficacy of Bimekizumab in Patients with Psoriatic Arthritis: 2-Year Results from Two Phase 3 Studies.Rheumatol Ther. 2025 Jun;12(3):597-599. doi: 10.1007/s40744-025-00761-x. Rheumatol Ther. 2025. PMID: 40323371 Free PMC article. No abstract available.
Abstract
Introduction: Psoriatic arthritis (PsA) is a chronic inflammatory disease requiring long-term treatment. Bimekizumab, a monoclonal IgG1 antibody that selectively inhibits interleukin (IL)-17F in addition to IL-17A, has demonstrated tolerability and sustained clinical efficacy for up to 1 year for patients with PsA. Here, we report the longer-term safety and efficacy of bimekizumab up to 2 years.
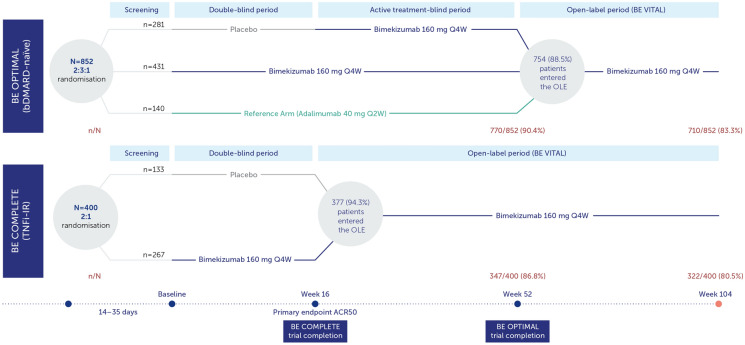
Methods: BE OPTIMAL (biologic disease-modifying antirheumatic drug [bDMARD]-naïve) and BE COMPLETE (prior inadequate response/intolerance to tumor necrosis factor inhibitors [TNFi-IR]) assessed subcutaneous bimekizumab 160 mg every 4 weeks in patients with PsA. BE OPTIMAL included a reference arm (adalimumab 40 mg every 2 weeks); patients switched to bimekizumab at week 52 with no washout between treatments. BE OPTIMAL week 52 and BE COMPLETE week 16 completers were eligible for the BE VITAL open-label extension. Efficacy outcomes are reported to week 104/100 (BE OPTIMAL/BE COMPLETE).
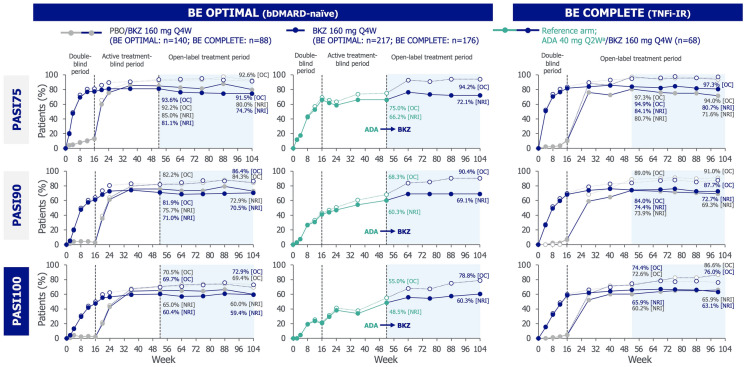
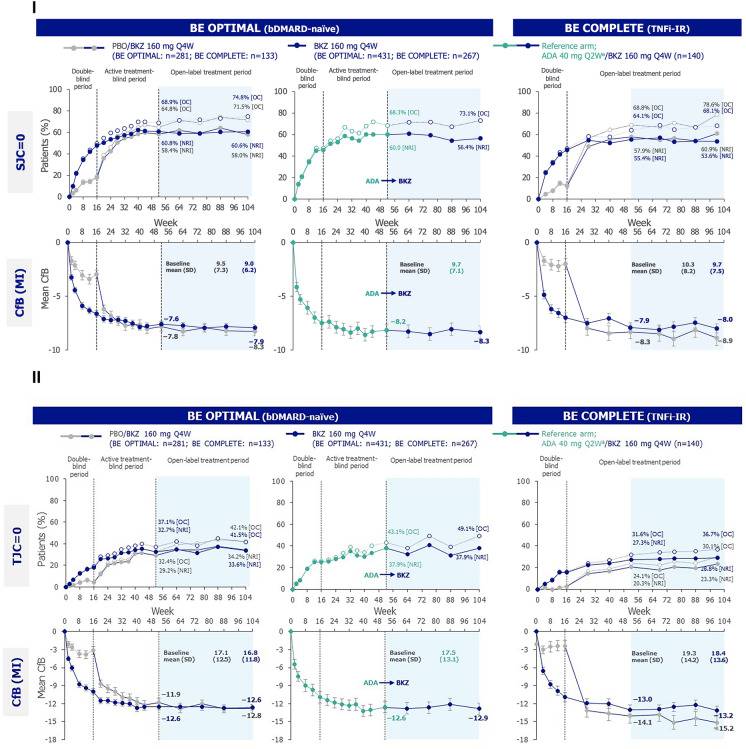
Results: A total of 710/852 (83.3%) bDMARD-naïve and 322/400 (80.5%) TNFi-IR patients completed week 104/100. Up to 104 weeks, patients treated with bimekizumab in BE OPTIMAL and BE COMPLETE had treatment-emergent adverse event incidence rates (exposure-adjusted incidence rate/100 patient-years) of 179.9 (95% CI 166.9, 193.7) and 100.3 (89.2, 112.4), respectively. The proportion of patients achieving efficacy outcomes (≥ 50% improvement from baseline in American College of Rheumatology [ACR] response criteria, 100% improvement from baseline in Psorisis Area and Severity Index [PASI], minimal disease activity [MDA]) was sustained in all patients from week 52 to week 104/100.
Conclusions: Bimekizumab was well tolerated for up to 2 years of treatment and no new safety signals were observed. Sustained clinical efficacy was observed up to 2 years in bDMARD-naïve and TNFi-IR patients with active PsA. Patients switching from adalimumab to bimekizumab demonstrated further improvement in skin and nail symptoms, and sustained efficacy in joint symptoms.
Trial registration: BE OPTIMAL (NCT03895203), BE COMPLETE (NCT03896581), BE VITAL (NCT04009499).
Keywords: Bimekizumab; Efficacy; Psoriatic arthritis; Safety; TNFi-inadequate responders; bDMARD-naïve.
© 2024. The Author(s).
Conflict of interest statement
Philip J. Mease: Received research grants from AbbVie, Acelyrin, Amgen, BMS, Eli Lilly, Janssen, Novartis, Pfizer and UCB Pharma; consulting fees from AbbVie, Acelyrin, Aclaris, Alumis, Amgen, BMS, Boehringer Ingelheim, Eli Lilly, Inmagene, Janssen, Moonlake Pharma, Novartis, Pfizer, Takeda, UCB Pharma and Ventyx; speakers bureau fees from AbbVie, Amgen, Eli Lilly, Janssen, Novartis, Pfizer and UCB Pharma; data safety and advisory board for Genascence. Joseph F. Merola: Is a consultant and/or investigator for AbbVie, Amgen, AstraZeneca, Biogen, Boehringer Ingelheim, Bristol-Myers Squibb, Dermavant, Eli Lilly, Incyte, Janssen, LEO Pharma, MoonLake Immunotherapeutics, Novartis, Pfizer, Sanofi-Regeneron, Sun Pharma and UCB Pharma. Joseph F. Merola’s current affiliation is “
Figures



References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
