

Biomarker-based prediction of sinus rhythm in atrial fibrillation patients: the EAST-AFNET 4 biomolecule study
- PMID: 39215973
- PMCID: PMC11646612
- DOI: 10.1093/eurheartj/ehae611
Biomarker-based prediction of sinus rhythm in atrial fibrillation patients: the EAST-AFNET 4 biomolecule study
Abstract
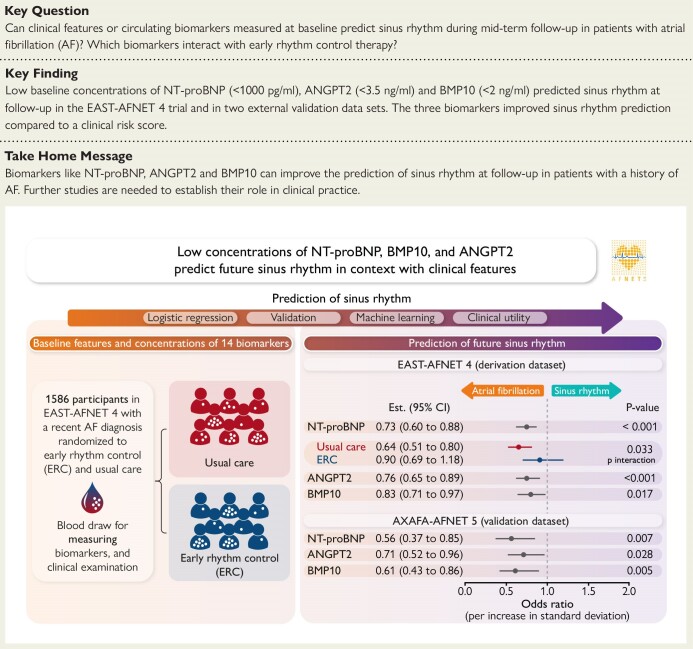
Background and aims: In patients with atrial fibrillation (AF), recurrent AF and sinus rhythm during follow-up are determined by interactions between cardiovascular disease processes and rhythm control therapy. Predictors of attaining sinus rhythm at follow-up are not well known.
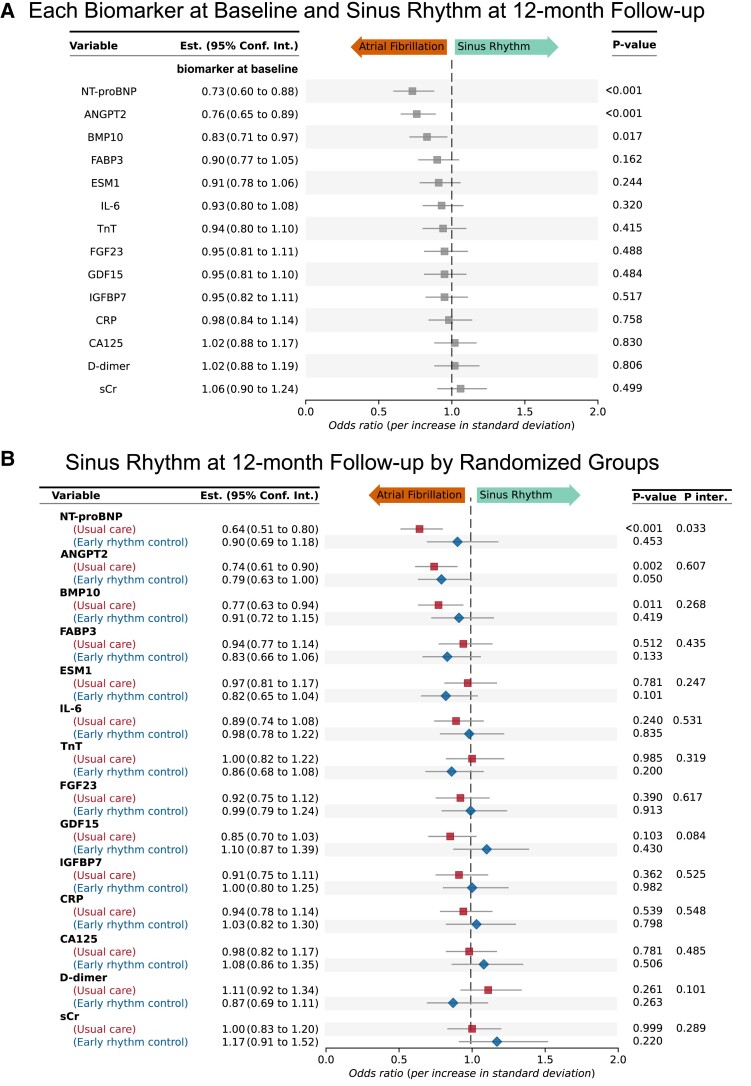
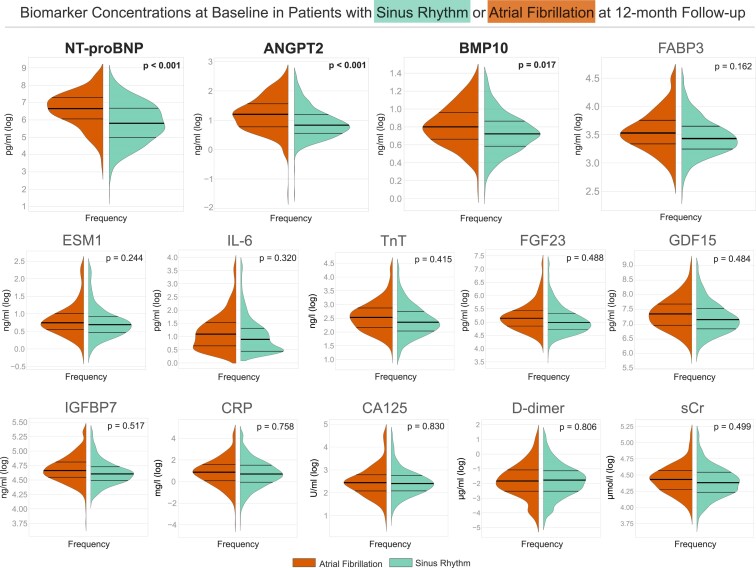
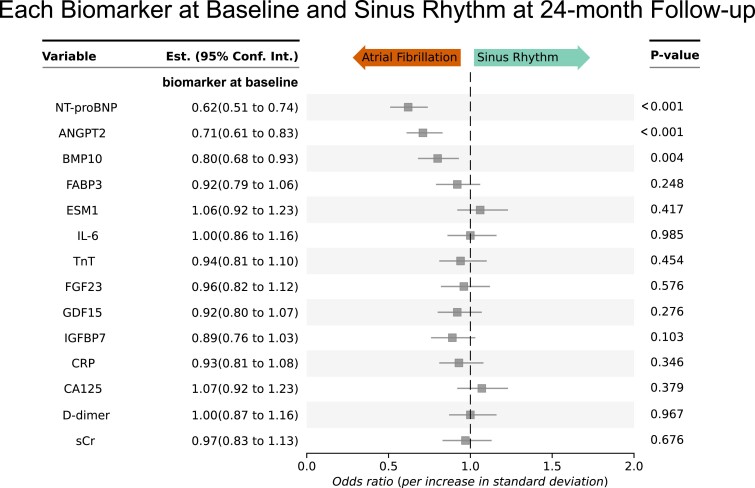
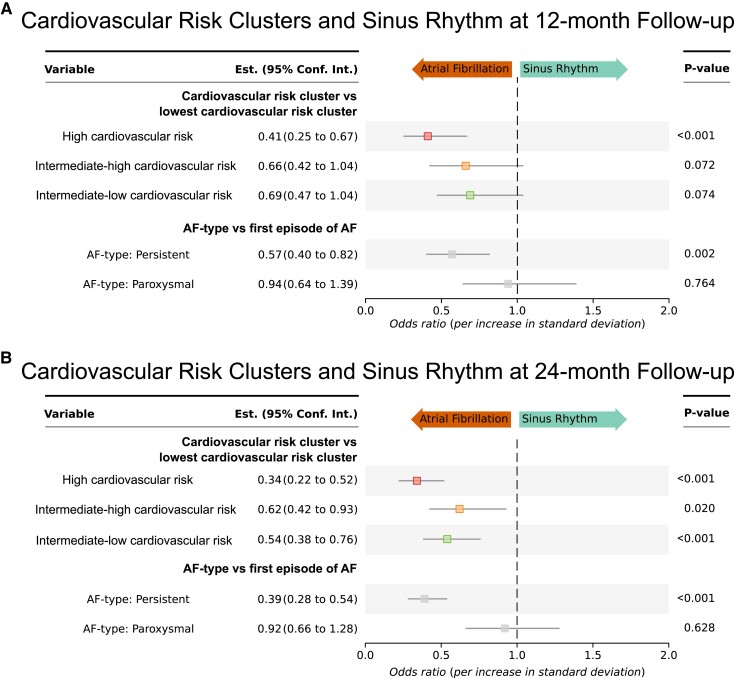
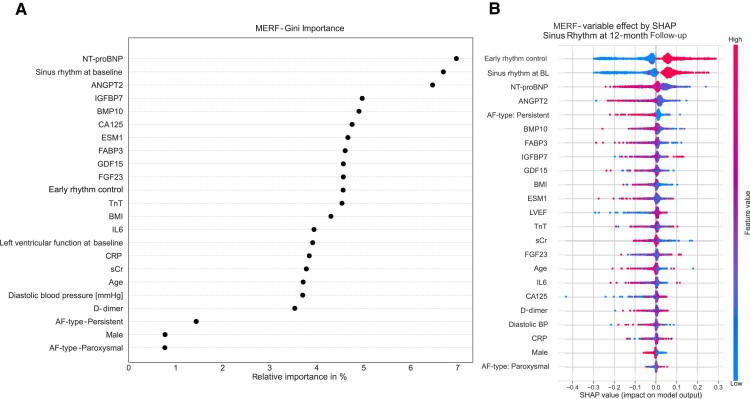
Methods: To quantify the interaction between cardiovascular disease processes and rhythm outcomes, 14 biomarkers reflecting AF-related cardiovascular disease processes in 1586 patients in the EAST-AFNET 4 biomolecule study (71 years old, 45% women) were quantified at baseline. Mixed logistic regression models including clinical features were constructed for each biomarker. Biomarkers were interrogated for interaction with early rhythm control. Outcome was sinus rhythm at 12 months. Results were validated at 24 months and in external datasets.
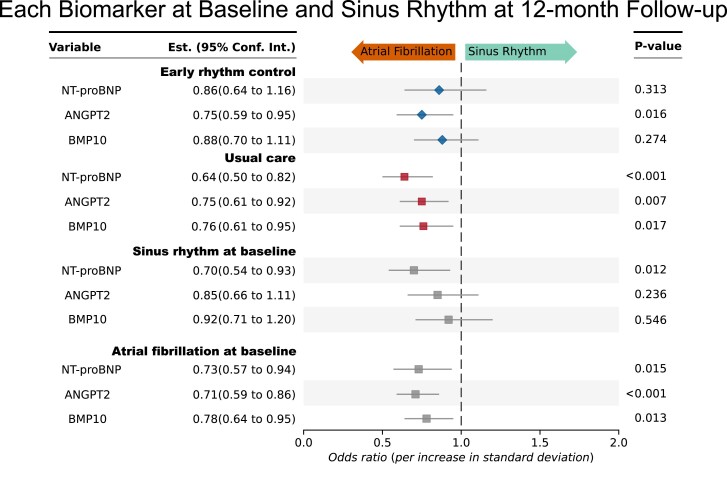
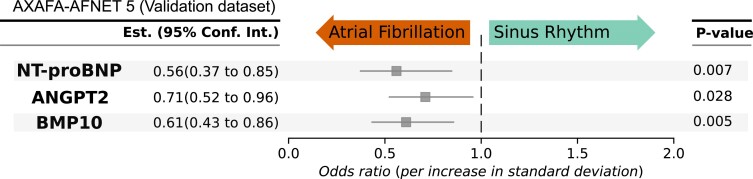
Results: Higher baseline concentrations of three biomarkers were independently associated with a lower chance of sinus rhythm at 12 months: angiopoietin 2 (ANGPT2) (odds ratio [OR] .76 [95% confidence interval .65-.89], P < .001), bone morphogenetic protein 10 (BMP10) (OR .83 [.71-.97], P = .017), and N-terminal pro-B-type natriuretic peptide (NT-proBNP) (OR .73 [.60-.88], P < .001). Analysis of rhythm at 24 months confirmed the results. Early rhythm control interacted with the predictive potential of NT-proBNP (Pinteraction = .033). The predictive effect of NT-proBNP was reduced in patients randomized to early rhythm control (usual care: OR .64 [.51-.80], P < .001; early rhythm control: OR .90 [.69-1.18], P = .453). External validation confirmed that low concentrations of ANGPT2, BMP10, and NT-proBNP predict sinus rhythm during follow-up.
Conclusions: Low concentrations of ANGPT2, BMP10, and NT-proBNP identify patients with AF who are likely to attain sinus rhythm during follow-up. The predictive ability of NT-proBNP is attenuated in patients receiving rhythm control.
Keywords: Angiopoietin 2; Atrial fibrillation; Blood biomarker; Bone morphogenetic protein 10; Natriuretic peptides; Rhythm control; Risk prediction; Risk score; Sinus rhythm.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021;42:373–498. 10.1093/eurheartj/ehaa612 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- Bundesministerium für Bildung und Forschung (BMBF)
- Deutsches Zentrum für Herz-Kreislauf-Forschung (DZHK)
- Atrial Fibrillation NETwork (AFNET)
- European Heart Rhythm Association (EHRA)
- St. Jude Medical-Abbott, Sanofi
- the German Heart Foundation
- PG/20/22/35093/BHF_/British Heart Foundation/United Kingdom
- FKZ 81X2800182/the German Ministry of Education and Research
- Ki 509167694/German Research Foundation
- Leducq Foundation
- the German Ministry of Education and Research
- CVON2014-09/Dutch Heart Foundation
- 648131/European Research Council (ERC)
- 847770/European Union's Horizon 2020 research and innovation programme
- 101095480/European Union's Horizon Europe research and innovation programme
- 81Z1710103/German Center for Cardiovascular Research
- 01ZX1408A/German Ministry of Research and Education
- Abbott Medical, Medtronic, Boston Scientific
- Johnson & Johnson
- German Heart Foundation, University of Hamburg and German Federal Ministry of Education and Research
- the German Ministry of Education and Research
LinkOut - more resources
Full Text Sources
Medical
Research Materials
