

Early prognosis prediction for non-variceal upper gastrointestinal bleeding in the intensive care unit: based on interpretable machine learning
- PMID: 39217369
- PMCID: PMC11365121
- DOI: 10.1186/s40001-024-02005-0
Early prognosis prediction for non-variceal upper gastrointestinal bleeding in the intensive care unit: based on interpretable machine learning
Abstract
Introduction: This study aims to construct a mortality prediction model for patients with non-variceal upper gastrointestinal bleeding (NVUGIB) in the intensive care unit (ICU), employing advanced machine learning algorithms. The goal is to identify high-risk populations early, contributing to a deeper understanding of patients with NVUGIB in the ICU.
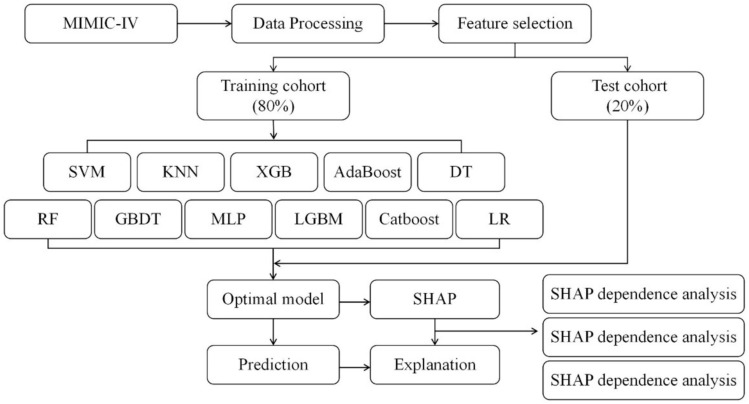
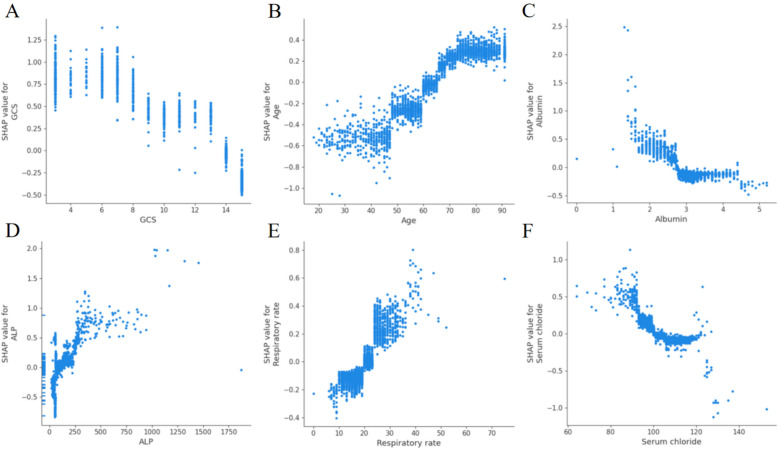
Methods: We extracted NVUGIB data from the Medical Information Mart for Intensive Care IV (MIMIC-IV, v.2.2) database spanning from 2008 to 2019. Feature selection was conducted through LASSO regression, followed by training models using 11 machine learning methods. The best model was chosen based on the area under the curve (AUC). Subsequently, Shapley additive explanations (SHAP) was employed to elucidate how each factor influenced the model. Finally, a case was randomly selected, and the model was utilized to predict its mortality, demonstrating the practical application of the developed model.
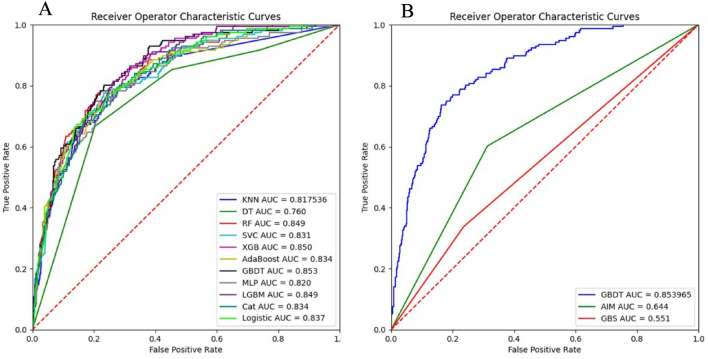
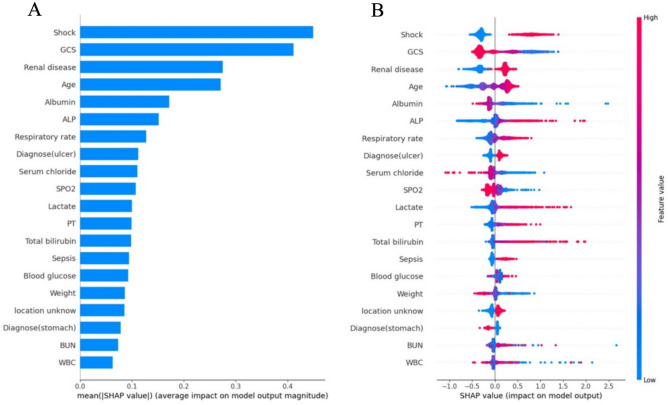
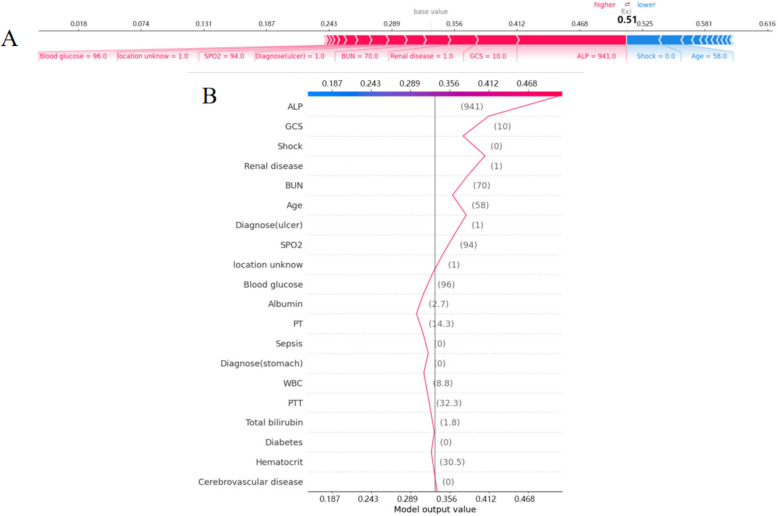
Results: In total, 2716 patients with NVUGIB were deemed eligible for participation. Following selection, 30 out of a total of 64 clinical parameters collected on day 1 after ICU admission remained associated with prognosis and were utilized for developing machine learning models. Among the 11 constructed models, the Gradient Boosting Decision Tree (GBDT) model demonstrated the best performance, achieving an AUC of 0.853 and an accuracy of 0.839 in the validation cohort. Feature importance analysis highlighted that shock, Glasgow Coma Scale (GCS), renal disease, age, albumin, and alanine aminotransferase (ALP) were the top six features of the GBDT model with the most significant impact. Furthermore, SHAP force analysis illustrated how the constructed model visualized the individualized prediction of death.
Conclusions: Patient data from the MIMIC database were leveraged to develop a robust prognostic model for patients with NVUGIB in the ICU. The analysis using SHAP also assisted clinicians in gaining a deeper understanding of the disease.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Interpretable machine learning for 28-day all-cause in-hospital mortality prediction in critically ill patients with heart failure combined with hypertension: A retrospective cohort study based on medical information mart for intensive care database-IV and eICU databases.Front Cardiovasc Med. 2022 Oct 12;9:994359. doi: 10.3389/fcvm.2022.994359. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36312291 Free PMC article.
-
Predicting sepsis in-hospital mortality with machine learning: a multi-center study using clinical and inflammatory biomarkers.Eur J Med Res. 2024 Mar 6;29(1):156. doi: 10.1186/s40001-024-01756-0. Eur J Med Res. 2024. PMID: 38448999 Free PMC article.
-
Interpretable Machine Learning for Early Prediction of Prognosis in Sepsis: A Discovery and Validation Study.Infect Dis Ther. 2022 Jun;11(3):1117-1132. doi: 10.1007/s40121-022-00628-6. Epub 2022 Apr 10. Infect Dis Ther. 2022. PMID: 35399146 Free PMC article.
-
The future of critical care: AI-powered mortality prediction for acute variceal gastrointestinal bleeding and acute non-variceal gastrointestinal bleeding patients.Front Med (Lausanne). 2025 May 16;12:1580094. doi: 10.3389/fmed.2025.1580094. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40454154 Free PMC article.
-
Mortality Prediction in the ICU.2016 Sep 10. In: MIT Critical Data, editor. Secondary Analysis of Electronic Health Records [Internet]. Cham (CH): Springer; 2016. Chapter 21. 2016 Sep 10. In: MIT Critical Data, editor. Secondary Analysis of Electronic Health Records [Internet]. Cham (CH): Springer; 2016. Chapter 21. PMID: 31314254 Free Books & Documents. Review.
Cited by
-
Association between international normalized ratio-to-albumin ratio and mortality in critically ill patients with gastrointestinal bleeding: a retrospective MIMIC-IV database study.BMC Gastroenterol. 2025 Aug 11;25(1):574. doi: 10.1186/s12876-025-04179-1. BMC Gastroenterol. 2025. PMID: 40790158 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
