

Acoustic-based rule-out of stable coronary artery disease: the FILTER-SCAD trial
- PMID: 39217444
- PMCID: PMC11704391
- DOI: 10.1093/eurheartj/ehae570
Acoustic-based rule-out of stable coronary artery disease: the FILTER-SCAD trial
Abstract
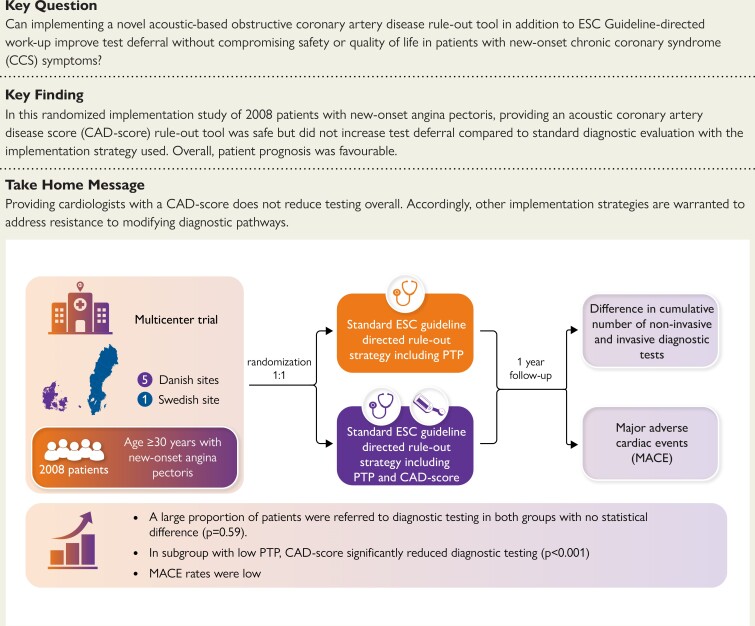
Background and aims: Overtesting of low-risk patients with suspect chronic coronary syndrome (CCS) is widespread. The acoustic-based coronary artery disease (CAD)-score has superior rule-out capabilities when added to pre-test probability (PTP). FILTER-SCAD tested whether providing a CAD-score and PTP to cardiologists was superior to PTP alone in limiting testing.
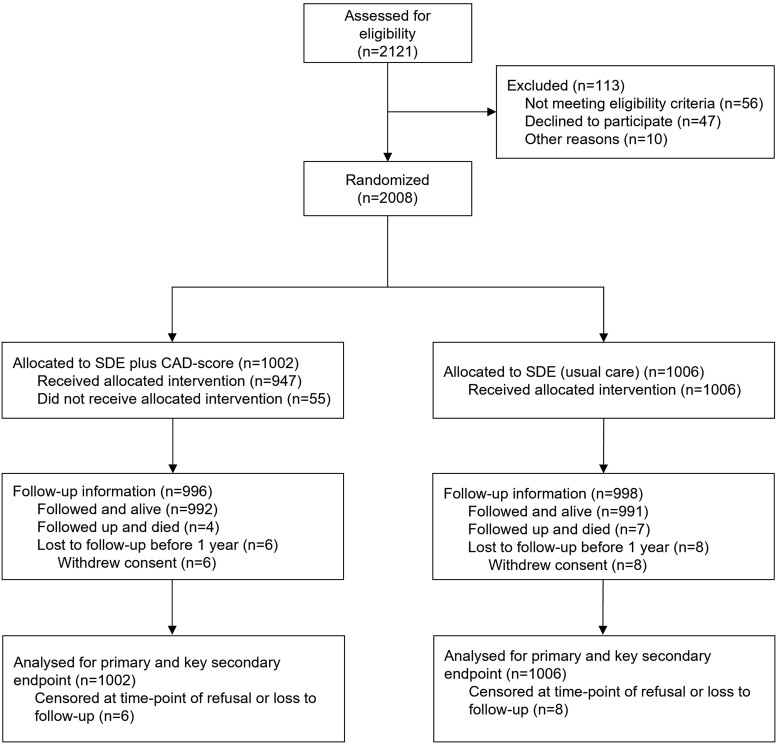
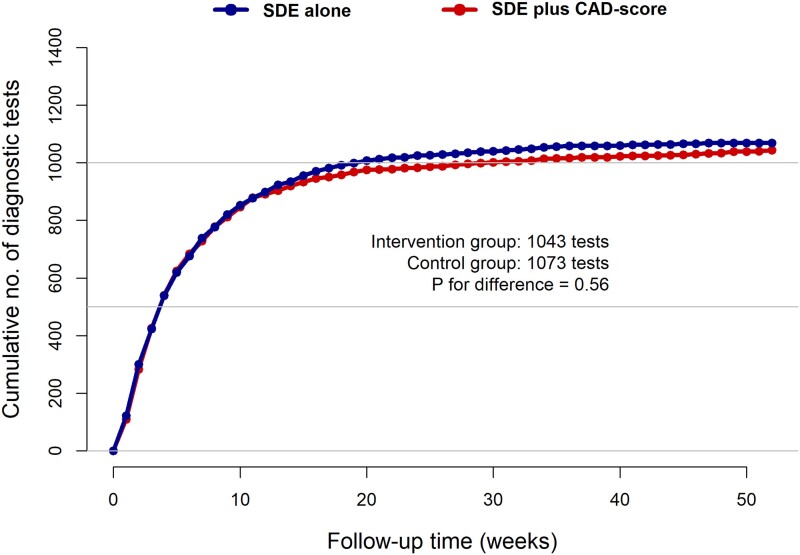
Methods: At six Danish and Swedish outpatient clinics, patients with suspected new-onset CCS were randomized to either standard diagnostic examination (SDE) with PTP, or SDE plus CAD-score, and cardiologists provided with corresponding recommended diagnostic flowcharts. The primary endpoint was cumulative number of diagnostic tests at one year and key safety endpoint major adverse cardiac events (MACE).
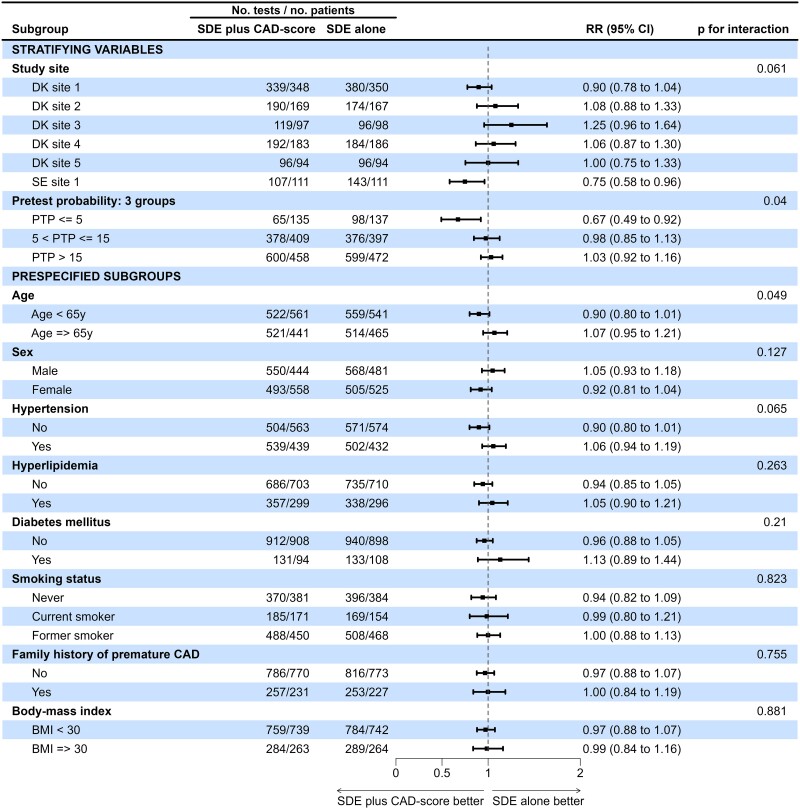
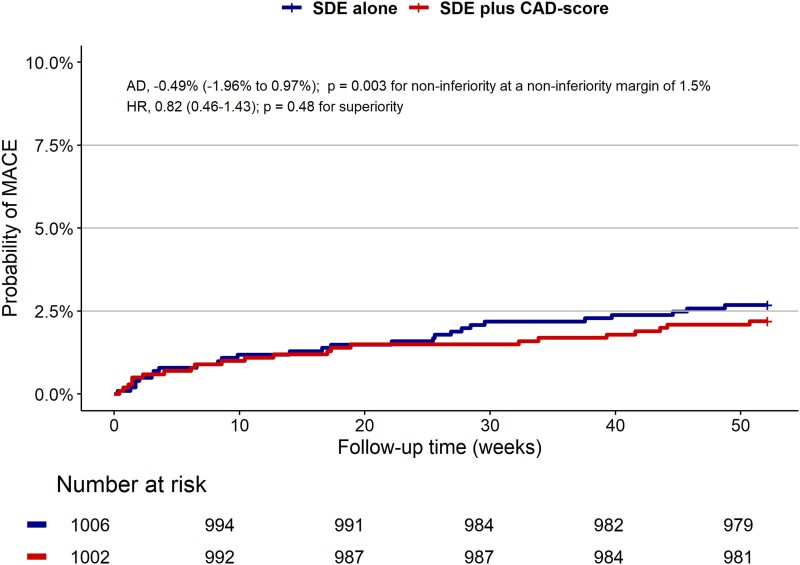
Results: In total, 2008 patients (46% male, median age 63 years) were randomized from October 2019 to September 2022. When randomized to CAD-score (n = 1002), it was successfully measured in 94.5%. Overall, 13.5% had PTP ≤ 5%, and 39.5% had CAD-score ≤ 20. Testing was deferred in 22% with no differences in diagnostic tests between groups (P for superiority = .56). In the PTP ≤ 5% subgroup, the proportion with deferred testing increased from 28% to 52% (P < .001). Overall MACE was 2.4 per 100 person-years. Non-inferiority regarding safety was established, absolute risk difference 0.49% (95% confidence interval -1.96-0.97) (P for non-inferiority = .003). No differences were seen in angina-related health status or quality of life.
Conclusions: The implementation strategy of providing cardiologists with a CAD-score alongside SDE did not reduce testing overall but indicated a possible role in patients with low CCS likelihood. Further strategies are warranted to address resistance to modifying diagnostic pathways in this patient population.
Keywords: Chronic coronary syndrome; Coronary artery disease; Deferred testing; Diagnostic strategy; Heart sound; Implementation strategy; Pre-test probability; Risk stratification.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
