

Effects of beta-blockers on quality of life and well-being in patients with myocardial infarction and preserved left ventricular function-a prespecified substudy from REDUCE-AMI
- PMID: 39217445
- PMCID: PMC11724137
- DOI: 10.1093/ehjcvp/pvae062
Effects of beta-blockers on quality of life and well-being in patients with myocardial infarction and preserved left ventricular function-a prespecified substudy from REDUCE-AMI
Abstract
Aims: In the Randomized Evaluation of Decreased Usage of Beta-Blockers after Acute Myocardial Infarction (REDUCE-AMI) study, long-term beta-blocker use in patients after acute myocardial infarction (AMI) with preserved left ventricular ejection fraction demonstrated no effect on death or cardiovascular outcomes. The aim of this prespecified substudy was to investigate effects of beta-blockers on self-reported quality of life and well-being.
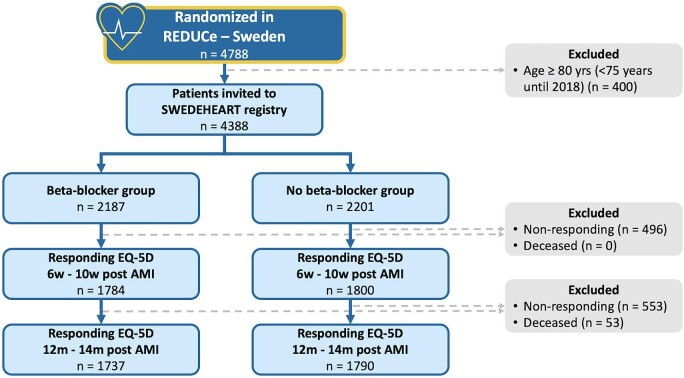
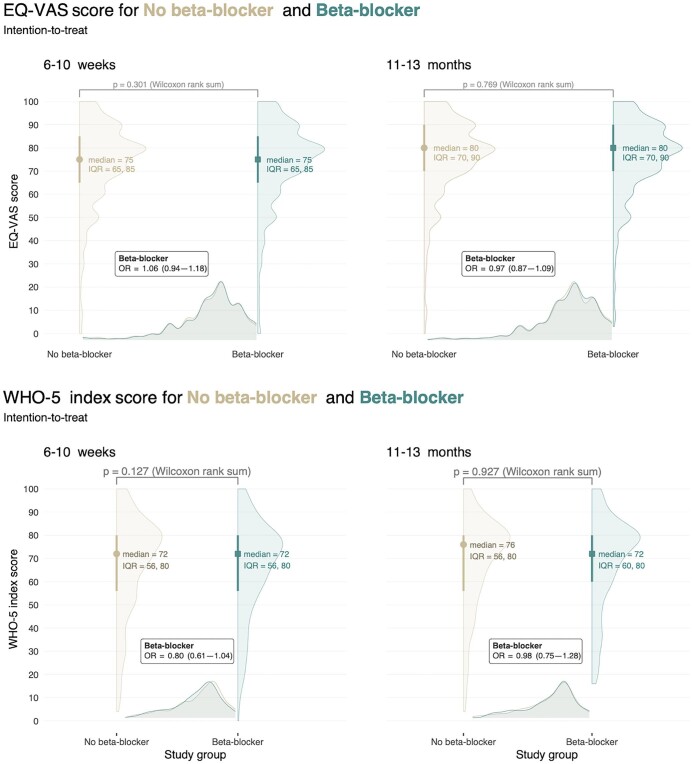
Methods and results: From this parallel-group, open-label, registry-based randomized clinical trial, EQ-5D, and World Health Organization well-being index-5 (WHO-5) questionnaires were obtained at 6-10 weeks and 11-13 months after AMI in 4080 and 806 patients, respectively. We report results from intention-to-treat and on-treatment analyses for the overall population and relevant subgroups using Wilcoxon rank sum test and adjusted ordinal regression analyses. Of the 4080 individuals reporting EQ-5D (median age 64 years, 22% female), 2023 were randomized to beta-blockers. The main outcome, median EQ-5D index score, was 0.94 [interquartile range (IQR) 0.88, 0.97] in the beta-blocker group, and 0.94 (IQR 0.88, 0.97) in the no-beta-blocker group 6-10 weeks after AMI, OR 1.00 [95% CI 0.89-1.13; P > 0.9]. After 11-13 months, results remained unchanged. Findings were robust in on-treatment analyses and across relevant subgroups. Secondary outcomes, EQ-VAS and WHO-5 index score, confirmed these results.
Conclusion: Among patients after AMI with preserved left ventricular ejection fraction, self-reported quality of life and well-being was not significantly different in individuals randomized to routine long-term beta-blocker therapy as compared to individuals with no beta-blocker use. These results appear consistent regardless of adherence to randomized treatment and across subgroups which emphasizes the need for a careful individual risk-benefit evaluation prior to initiation of beta-blocker treatment.
Keywords: AMI: Acute myocardial infarction; EQ-5D: EuroQoL 5-dimension; EQ-VAS: EuroQoL visual analogue scale; LVEF: Left ventricular ejection fraction; QoL: Quality of life; SWEDEHEART: Swedish Web System for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies; WHO-5: World Health Organization-5.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures



References
-
- Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, Claeys MJ, Dan G-A, Dweck MR, Galbraith M, Gilard M, Hinterbuchner L, Jankowska EA, Jüni P, Kimura T, Kunadian V, Leosdottir M, Lorusso R, Pedretti RFE, Rigopoulos AG, Rubini Gimenez M, Thiele H, Vranckx P, Wassmann S, Wenger NK, Ibanez B, Halvorsen S, James S, Abdelhamid M, Aboyans V, Marsan NA, Antoniou S, Asteggiano R, Bäck M, Capodanno D, Casado-Arroyo R, Cassese S, Čelutkienė J, Cikes M, Collet J-P, Ducrocq G, Falk V, Fauchier L, Geisler T, Gorog DA, Holmvang L, Jaarsma T, Jones HW, Køber L, Koskinas KC, Kotecha D, Krychtiuk KA, Landmesser U, Lazaros G, Lewis BS, Lindahl B, Linhart A, Løchen M-L, Mamas MA, Mcevoy JW, Mihaylova B, Mindham R, Mueller C, Neubeck L, Niebauer J, Nielsen JC, Niessner A, Paradies V, Pasquet AA, Petersen SE, Prescott E, Rakisheva A, Rocca B, Rosano GMC, Sade LE, Schiele F, Siller-Matula JM, Sticherling C, Storey RF, Thielmann M, Vrints C, Windecker S, Wiseth R, Witkowski A, El Amine Bouzid M, Hayrapetyan H, Metzler B, Lancellotti P, Bajrić M, Karamfiloff K, Mitsis A, Ostadal P, Sørensen R, Elwasify T, Marandi T, Ryödi E, Collet J-P, Chukhrukidze A, Mehilli J, Davlouros P, Becker D, Guðmundsdóttir IJ, Crowley J, Abramowitz Y, Indolfi C, Sakhov O, Elezi S, Beishenkulov M, Erglis A, Moussallem N, Benlamin H, Dobilienė O, Degrell P, Balbi MM, Grosu A, Lakhal Z, Ten Berg J, Pejkov H, Angel K, Witkowski A, De Sousa Almeida M, Chioncel O, Bertelli L, Stojkovic S, Studenčan M, Radšel P, Ferreiro JL, Ravn-Fischer A, Räber L, Marjeh MYB, Hassine M, Yildirir A, Parkhomenko A, Banning AP, Prescott E, James S, Arbelo E, Baigent C, Borger MA, Buccheri S, Ibanez B, Køber L, Koskinas KC, Mcevoy JW, Mihaylova B, Mindham R, Neubeck L, Nielsen JC, Pasquet AA, Rakisheva A, Rocca B, Rossello X, Vaartjes I, Vrints C, Witkowski A, Zeppenfeld K. 2023 ESC Guidelines for the management of acute coronary syndromes: developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J 2023;44:3720–3826. - PubMed
-
- Norwegian Multicenter Study Group . Timolol-induced reduction in mortality and reinfarction in patients surviving acute myocardial infarction. N Engl J Med 1981;304:801–807. - PubMed
-
- National Heart, Lung, and Blood Institute. A randomized trial of propranolol in patients with acute myocardial infarction. I. Mortality results. J Am Med Assoc 1982;247:1707–1714. - PubMed
-
- Metoprolol in acute myocardial infarction (MIAMI) . A randomised placebo-controlled international trial. The MIAMI Trial Research Group. Eur Heart J 1985;6:199–226. - PubMed
-
- Hjalmarson Å, Herlitz J, Málek I, Rydén L, Vedin A, Waldenström A, Wedel H, Elmfeldt D, Holmberg S, Nyberg G, Swedberg K, Waagstein F, Waldenström J, Wilhelmsen L, Wilhelmsson C. Effect on mortality of metoprolol in acute myocardial infarction. A double-blind randomised trial. Lancet 1981;2:823–827. - PubMed
