

Gender and contemporary risk of adverse events in atrial fibrillation
- PMID: 39217497
- PMCID: PMC11439109
- DOI: 10.1093/eurheartj/ehae539
Gender and contemporary risk of adverse events in atrial fibrillation
Abstract
Background and aims: The role of gender in decision-making for oral anticoagulation in patients with atrial fibrillation (AF) remains controversial.
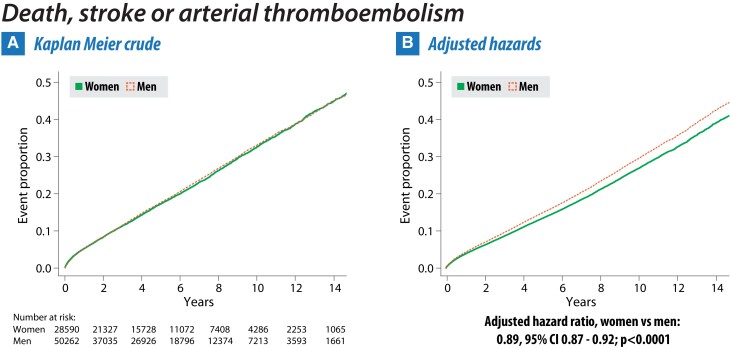
Methods: The population cohort study used electronic healthcare records of 16 587 749 patients from UK primary care (2005-2020). Primary (composite of all-cause mortality, ischaemic stroke, or arterial thromboembolism) and secondary outcomes were analysed using Cox hazard ratios (HR), adjusted for age, socioeconomic status, and comorbidities.
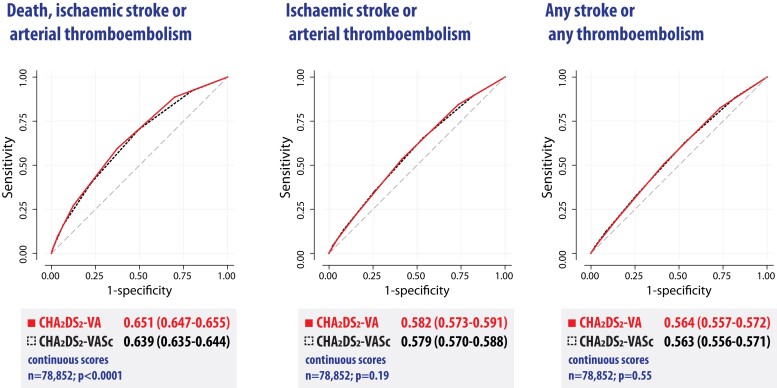
Results: 78 852 patients were included with AF, aged 40-75 years, no prior stroke, and no prescription of oral anticoagulants. 28 590 (36.3%) were women, and 50 262 (63.7%) men. Median age was 65.7 years (interquartile range 58.5-70.9), with women being older and having other differences in comorbidities. During a total follow-up of 431 086 patient-years, women had a lower adjusted primary outcome rate with HR 0.89 vs. men (95% confidence interval [CI] 0.87-0.92; P < .001) and HR 0.87 after censoring for oral anticoagulation (95% CI 0.83-0.91; P < .001). This was driven by lower mortality in women (HR 0.86, 95% CI 0.83-0.89; P < .001). No difference was identified between women and men for the secondary outcomes of ischaemic stroke or arterial thromboembolism (adjusted HR 1.00, 95% CI 0.94-1.07; P = .87), any stroke or any thromboembolism (adjusted HR 1.02, 95% CI 0.96-1.07; P = .58), and incident vascular dementia (adjusted HR 1.13, 95% CI 0.97-1.32; P = .11). Clinical risk scores were only modest predictors of outcomes, with CHA2DS2-VA (ignoring gender) superior to CHA2DS2-VASc for primary outcomes in this population (receiver operating characteristic curve area 0.651 vs. 0.639; P < .001) and no interaction with gender (P = .45).
Conclusions: Removal of gender from clinical risk scoring could simplify the approach to which patients with AF should be offered oral anticoagulation.
Keywords: Atrial fibrillation; Gender; Sex; Stroke; Thromboembolism; Women.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures




References
-
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJGM. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on Atrial Fibrillation. Chest 2010;137:263–72. 10.1378/chest.09-1584 - DOI - PubMed
-
- Fox KAA, Lucas JE, Pieper KS, Bassand J-P, Camm AJ, Fitzmaurice DA, et al. Improved risk stratification of patients with atrial fibrillation: an integrated GARFIELD-AF tool for the prediction of mortality, stroke and bleed in patients with and without anticoagulation. BMJ Open 2017;7:e017157. 10.1136/bmjopen-2017-017157 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
