

From drug therapy failures to laser therapy victory: A case report and literature review of lupus miliaris disseminatus faciei resolution
- PMID: 39219778
- PMCID: PMC11364779
- DOI: 10.1002/ccr3.9370
From drug therapy failures to laser therapy victory: A case report and literature review of lupus miliaris disseminatus faciei resolution
Abstract
Key clinical message: Pulsed dye laser (PDL) has proven effective in resolving lupus miliaris disseminatus faciei (LMDF) where drug therapies have failed with a lack of treatment consensus for LMDF, considering early PDL intervention is crucial to achieve resolution without scarring, prevent relapse, and enhance overall treatment outcomes.
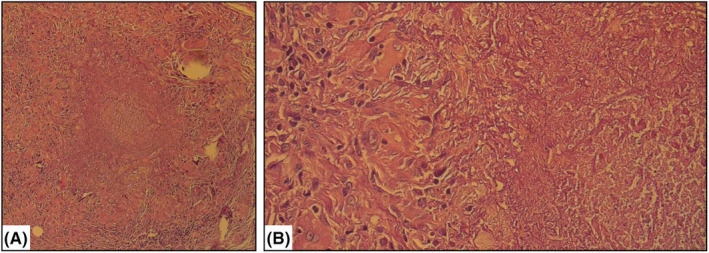
Abstract: Lupus miliaris disseminatus faciei (LMDF) is a rare inflammatory and granulomatous dermatologic disease that primarily affects the face. The optimal treatment for LMDF remains controversial, and there is a lack of consensus on the most effective therapy. This case report highlights the successful use of a 595 nm pulsed dye laser (PDL) in the treatment of LMDF following unsuccessful drug therapy. A 28-year-old male presented with reddish-brown eruptions on his face that had persisted for several months. Clinical examination revealed discrete dome-shaped eruptions in clusters on the central area of the face. Histopathological examination confirmed the diagnosis of LMDF, based on the presence of epithelioid granulomas with central caseous necrosis. Previous treatment with an oral isotretinoin and methotrexate combination also failed to yield satisfactory results. After discontinuing drug therapy, the patient underwent five sessions of PDL treatment. Ten days after the first session, the eruptions began to regress without scarring. Subsequent PDL sessions led to the complete resolution of the eruptions. The patient experienced no relapse during the follow-up period. This case report suggests that PDL treatment may be an effective option for LMDF, particularly in cases where drug therapy has failed. Early initiation of laser treatment may prevent scarring, minimize the adverse effects associated with drug therapy, and reduce the risk of disease relapse. Further research and controlled trials are needed to establish the efficacy of laser therapy in the treatment of LMDF.
Keywords: LMDF; acne agminata; granulomatous dermatosis; lupus miliaris disseminatus faciei; pulsed dye laser.
© 2024 The Author(s). Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
Lupus Miliaris Disseminatus Faciei versus Granulomatous Rosacea: A Case Report.Case Rep Dermatol. 2021 Jun 21;13(2):321-329. doi: 10.1159/000517209. eCollection 2021 May-Aug. Case Rep Dermatol. 2021. PMID: 34248540 Free PMC article.
-
Lupus Miliaris Disseminatus Faciei: A Report of a Rare Case and Its Differential Diagnosis.Cureus. 2024 Jun 26;16(6):e63245. doi: 10.7759/cureus.63245. eCollection 2024 Jun. Cureus. 2024. PMID: 39070463 Free PMC article.
-
A case of lupus miliaris disseminatus faciei that was successfully treated with 595 nm pulsed-dye laser combined with drugs.Dermatol Ther. 2020 May;33(3):e13373. doi: 10.1111/dth.13373. Epub 2020 Apr 17. Dermatol Ther. 2020. PMID: 32246556
-
Clinical and Histopathological Insights Into Lupus Miliaris Disseminatus Faciei: A Review of 70 Cases.J Cutan Pathol. 2025 May;52(5):386-391. doi: 10.1111/cup.14796. Epub 2025 Feb 13. J Cutan Pathol. 2025. PMID: 39945109 Review.
-
[Lupus miliaris disseminatus faciei associated with epidermal cysts].Actas Dermosifiliogr. 2005 Jun;96(5):320-2. doi: 10.1016/s0001-7310(05)75064-x. Actas Dermosifiliogr. 2005. PMID: 16476397 Review. Spanish.
Cited by
-
Systematic review of vascular lasers for the treatment of inflammatory active acne vulgaris.Lasers Med Sci. 2025 Apr 1;40(1):168. doi: 10.1007/s10103-025-04429-4. Lasers Med Sci. 2025. PMID: 40167813
References
-
- Skowron F, Causeret AS, Pabion C, Viallard AM, Balme B, Thomas L. F.I.GU.R.E.: facial idiopathic granulomas with regressive evolution. Is ‘lupus miliaris disseminatus faciei’ still an acceptable diagnosis in the third millennium? Dermatology. 2000;201(4):287‐289. doi:10.1159/000051539 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
