

Impact of mechanical circulatory support on out-of-hospital cardiac arrest outcomes stratified by vasoactive-inotropic score: A retrospective cohort study
- PMID: 39219812
- PMCID: PMC11363560
- DOI: 10.1016/j.resplu.2024.100743
Impact of mechanical circulatory support on out-of-hospital cardiac arrest outcomes stratified by vasoactive-inotropic score: A retrospective cohort study
Abstract
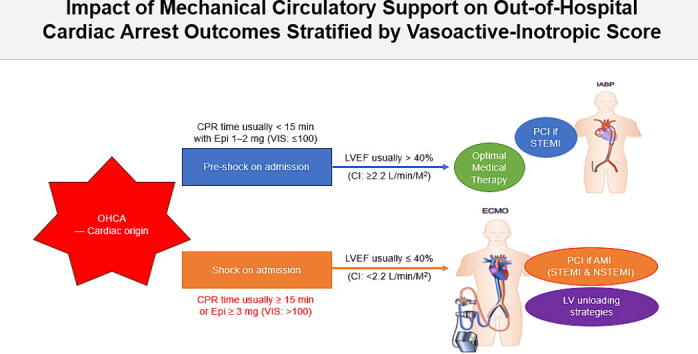
Aims: To assess whether mechanical circulatory support (MCS), including intra-aortic balloon pump (IABP) or veno-arterial extracorporeal membrane oxygenation (ECMO), can help improve neurological outcomes in patients with out-of-hospital cardiac arrest (OHCA).
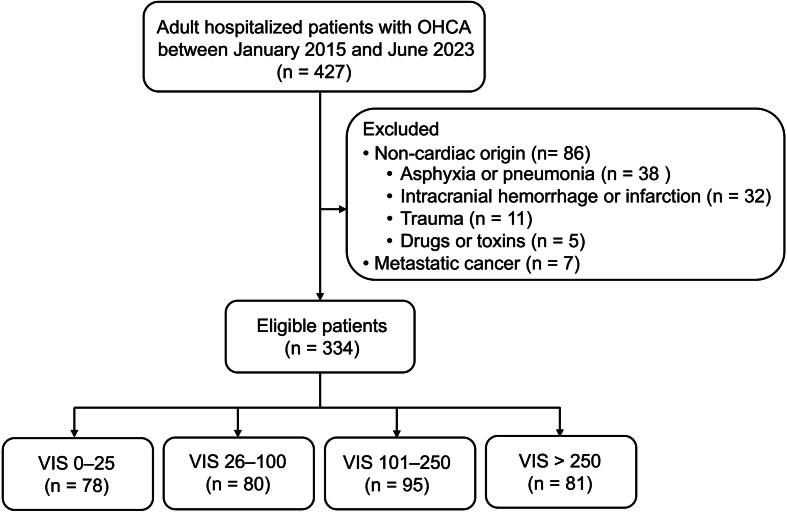
Methods: This is a retrospective observational cohort study performed in China Medical University Hospital, Taichung, Taiwan. Adult patients with OHCA admitted between January 2015 and June 2023. Quantitative score of vasoactive-inotropic agents and qualitative interventions of MCS, including IABP and ECMO after OHCA. Multivariate regression evaluated the efficacy of each MCS approach in patients stratified by the vasoactive-inotropic score (VIS).
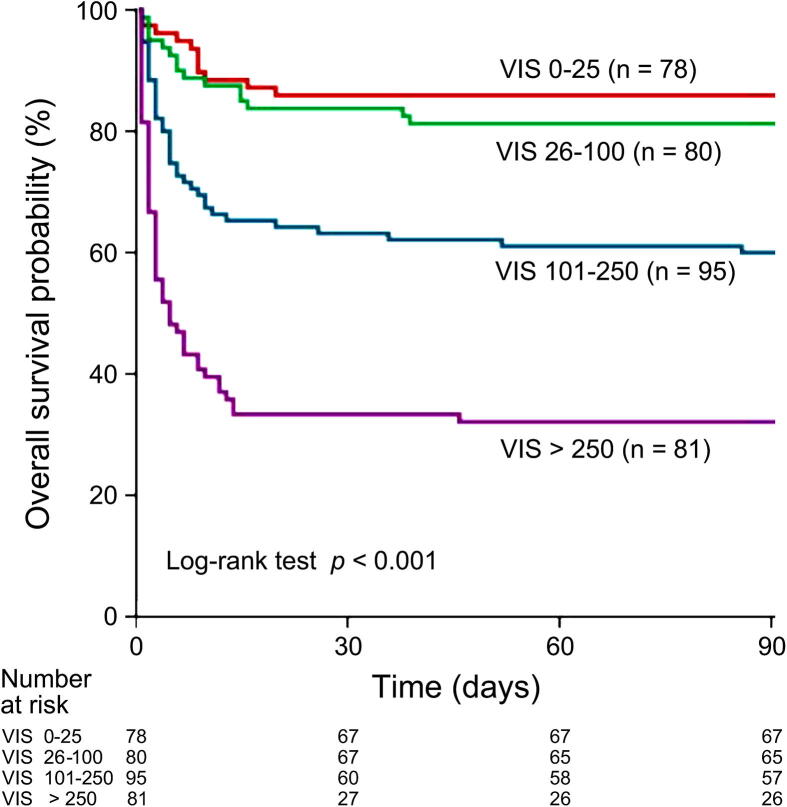
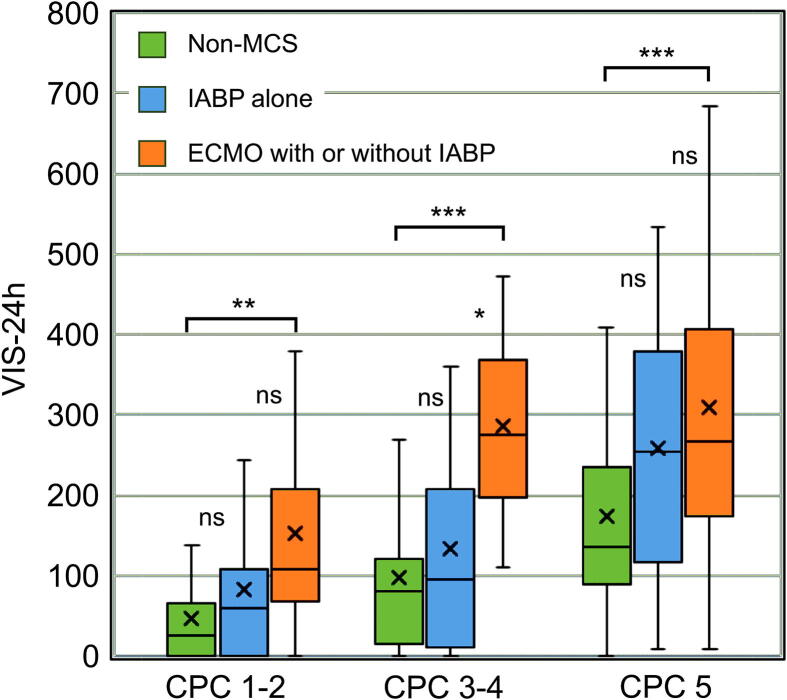
Results: A total of 334 patients were included and analyzed, 122 (36.5%) had favorable neurological outcomes and 215 (64.4%) survived ≥90 days. These patients were stratified by VIS: 0-25, 26-100, 101-250, and >250. In patients with a VIS > 100, ECMO with or without IABP ensured favorable neurological outcomes and survival after OHCA compared to non-MCS interventions (p < 0.001). For patients with a VIS ≤ 100, IABP alone was beneficial, with no significant outcome difference from non-MCS interventions (p > 0.05).
Conclusions: ECMO with or without IABP therapy may improve post-OHCA neurological outcomes and survival in patients with an expected VIS-24 h > 100 (e.g., epinephrine dose reaches 3 mg during CPR).
Keywords: Extracorporeal membrane oxygenation; Intra-aortic balloon pump; Mechanical circulatory support; Out-of-hospital cardiac arrest; Vasoactive-inotropic score.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Impact of extracorporeal CPR with transcatheter heart pump support (ECPELLA) on improvement of short-term survival and neurological outcome in patients with refractory cardiac arrest - A single-site retrospective cohort study.Resusc Plus. 2022 May 20;10:100244. doi: 10.1016/j.resplu.2022.100244. eCollection 2022 Jun. Resusc Plus. 2022. PMID: 35620182 Free PMC article.
-
Differential Prognostic Implications of Vasoactive Inotropic Score for Patients With Acute Myocardial Infarction Complicated by Cardiogenic Shock According to Use of Mechanical Circulatory Support.Crit Care Med. 2021 May 1;49(5):770-780. doi: 10.1097/CCM.0000000000004815. Crit Care Med. 2021. PMID: 33590998
-
Intra-aortic balloon pump and survival with favorable neurological outcome after out-of-hospital cardiac arrest: A multicenter, prospective propensity score-matched study.Resuscitation. 2019 Oct;143:165-172. doi: 10.1016/j.resuscitation.2019.07.002. Epub 2019 Jul 11. Resuscitation. 2019. PMID: 31302105
-
Extracorporeal Membrane Oxygenation for Cardiac Indications in Adults: A Health Technology Assessment.Ont Health Technol Assess Ser. 2020 Mar 6;20(8):1-121. eCollection 2020. Ont Health Technol Assess Ser. 2020. PMID: 32284771 Free PMC article.
-
Concomitant Intra-Aortic Balloon Pump Use in Cardiogenic Shock Requiring Veno-Arterial Extracorporeal Membrane Oxygenation.Circ Cardiovasc Interv. 2018 Sep;11(9):e006930. doi: 10.1161/CIRCINTERVENTIONS.118.006930. Circ Cardiovasc Interv. 2018. PMID: 30354593
References
LinkOut - more resources
Full Text Sources
