

Frequent Alzheimer's disease neuropathological change in patients with glioblastoma
- PMID: 39220249
- PMCID: PMC11362848
- DOI: 10.1093/noajnl/vdae118
Frequent Alzheimer's disease neuropathological change in patients with glioblastoma
Abstract
Background: The incidence of brain cancer and neurodegenerative diseases is increasing with a demographic shift towards aging populations. Biological parallels have been observed between glioblastoma and Alzheimer's disease (AD), which converge on accelerated brain aging. Here, we aimed to map the cooccurrence of AD neuropathological change (ADNC) in the tumor-adjacent cortex of patients with glioblastoma.
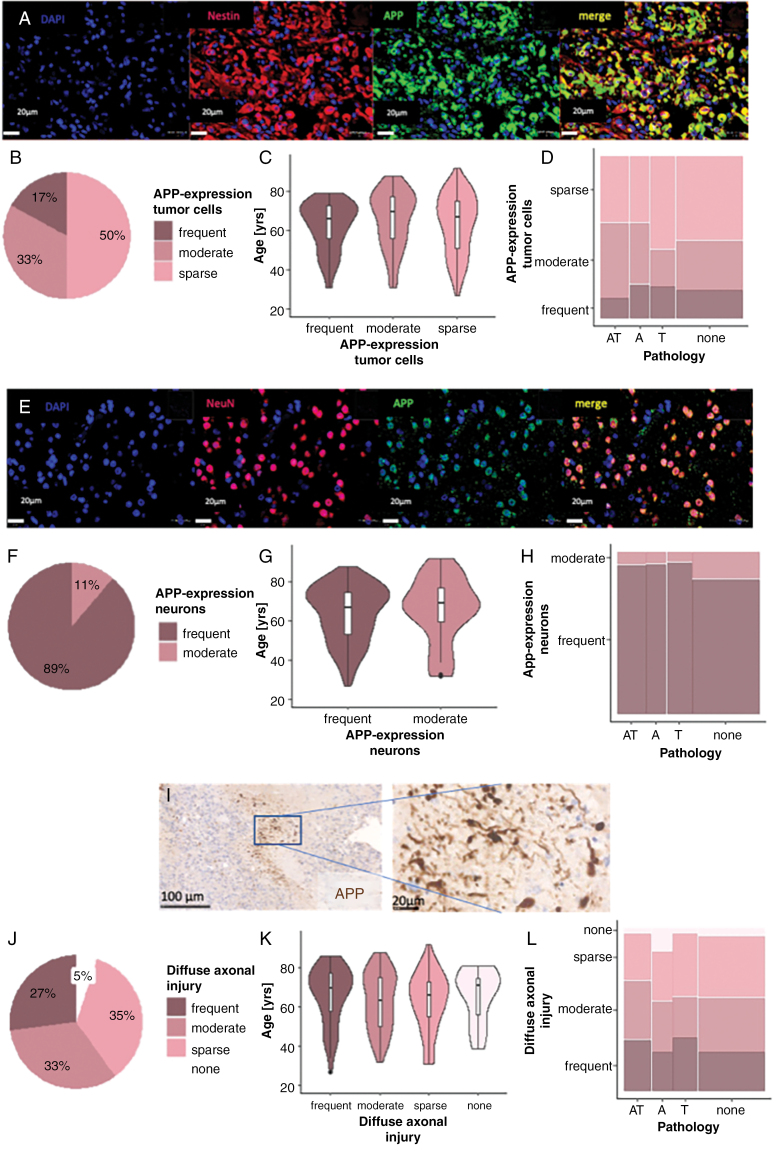
Methods: Immunohistochemical screening of AD markers amyloid beta (Abeta), amyloid precursor protein (APP), and hyperphosphorylated tau (pTau) was conducted in 420 tumor samples of 205 patients. For each cortex area, we quantified ADNC, neurons, tumor cells, and microglia.
Results: Fifty-two percent of patients (N = 106/205) showed ADNC (Abeta and pTau, Abeta or pTau) in the tumor-adjacent cortex, with histological patterns widely consistent with AD. ADNC was positively correlated with patient age and varied spatially according to Thal phases and Braak stages. It decreased with increasing tumor cell infiltration (P < .0001) and was independent of frequent expression of APP in neuronal cell bodies (N = 182/205) and in tumor necrosis-related axonal spheroids (N = 195/205; P = .46). Microglia response was most present in tumor cell infiltration plus ADNC, being further modulated by patient age and sex. ADNC did not impact patient survival in the present cohort.
Conclusions: Our findings highlight the frequent presence of ADNC in the glioblastoma vicinity, which was linked to patient age and tumor location. The cooccurrence of AD and glioblastoma seemed stochastic without clear spatial relation. ADNC did not impact patient survival in our cohort.
Keywords: Alzheimer’s disease; amyloid beta; brain aging; glioblastoma; hyperphosphorylated tau.
© The Author(s) 2024. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- 2023 Alzheimer’s disease facts and figures. Alzheimers Dement. 2023;19(4):1598–1695. - PubMed
LinkOut - more resources
Full Text Sources