

Genome-wide association study of susceptibility to hospitalised respiratory infections
- PMID: 39220670
- PMCID: PMC11362726
- DOI: 10.12688/wellcomeopenres.17230.2
Genome-wide association study of susceptibility to hospitalised respiratory infections
Abstract
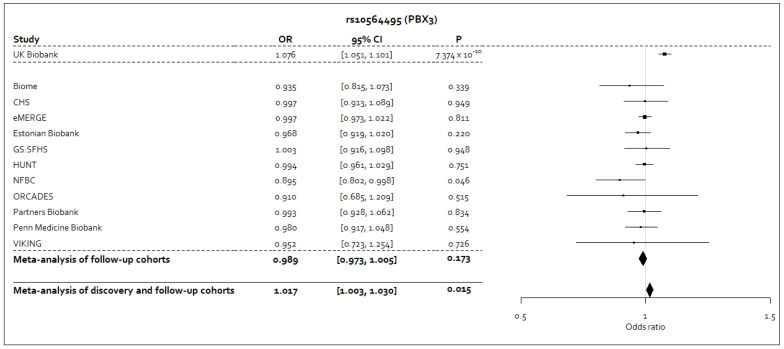
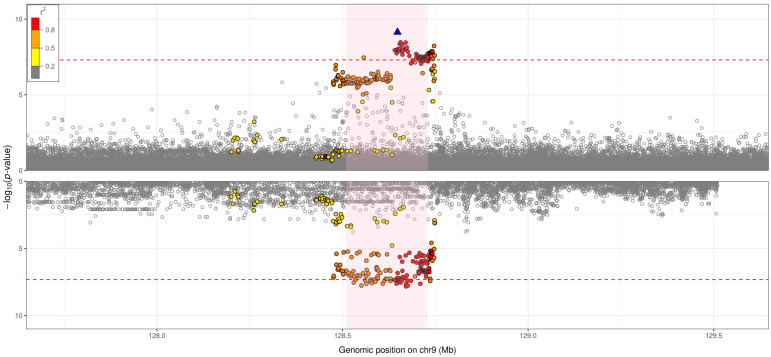
Background: Globally, respiratory infections contribute to significant morbidity and mortality. However, genetic determinants of respiratory infections are understudied and remain poorly understood. Methods: We conducted a genome-wide association study in 19,459 hospitalised respiratory infection cases and 101,438 controls from UK Biobank (Stage 1). We followed-up well-imputed top signals from our Stage 1 analysis in 50,912 respiratory infection cases and 150,442 controls from 11 cohorts (Stage 2). We aggregated effect estimates across studies using inverse variance-weighted meta-analyses. Additionally, we investigated the function of the top signals in order to gain understanding of the underlying biological mechanisms. Results: From our Stage 1 analysis, we report 56 signals at P<5×10 -6, one of which was genome-wide significant ( P<5×10 -8). The genome-wide significant signal was in an intron of PBX3, a gene that encodes pre-B-cell leukaemia transcription factor 3, a homeodomain-containing transcription factor. Further, the genome-wide significant signal was found to colocalise with gene-specific expression quantitative trait loci (eQTLs) affecting expression of PBX3 in lung tissue, where the respiratory infection risk alleles were associated with decreased PBX3 expression in lung tissue, highlighting a possible biological mechanism. Of the 56 signals, 40 were well-imputed in UK Biobank and were investigated in Stage 2. None of the 40 signals replicated, with effect estimates attenuated. Conclusions: Our Stage 1 analysis implicated PBX3 as a candidate causal gene and suggests a possible role of transcription factor binding activity in respiratory infection susceptibility. However, the PBX3 signal, and the other well-imputed signals, did not replicate in the meta-analysis of Stages 1 and 2. Significant phenotypic heterogeneity and differences in study ascertainment may have contributed to this lack of statistical replication. Overall, our study highlighted putative associations and possible biological mechanisms that may provide insight into respiratory infection susceptibility.
Keywords: GWAS; Respiratory infections; UK Biobank; electronic medical records.
Copyright: © 2023 Williams AT et al.
Conflict of interest statement
Competing interests: IPH has funded research collaborations with GSK, Boehringer Ingelheim and Orion. LVW and MDT receive funding from GSK for a collaborative research project outside of the submitted work. JCB, AJY and HNG are employees of GSK and may own company stock. At the time of this study, DM, SHL, HM and EMH were employees of GSK and may own company stock. MHC has received grant support from GSK and Bayer, consulting or speaking fees from Genentech, AstraZeneca, and Illumina, outside of the submitted work.
Figures


References
-
- Dasaraju PV, Liu C: Infections of the Respiratory System.In: Baron S, editor. Medical Microbiology. 4th edition, Galveston (TX): University of Texas Medical Branch at Galveston;1996; Chapter 93. Reference Source - PubMed
-
- GBD 2016 Causes of Death Collaborators: Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016.[published correction appears in Lancet. 2017 Oct 28; 390(10106):e38]. Lancet. 2017;390(10100):1151–1210. 10.1016/S0140-6736(17)32152-9 - DOI - PMC - PubMed
-
- GBD 2016 Lower Respiratory Infections Collaborators: Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1191–1210. 10.1016/S1473-3099(18)30310-4 - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
