

Finite Element Analysis of Protective Measures against Lateral Hinge Fractures in High-Tibial Osteotomy
- PMID: 39220812
- PMCID: PMC11362574
- DOI: 10.1155/2024/5510319
Finite Element Analysis of Protective Measures against Lateral Hinge Fractures in High-Tibial Osteotomy
Abstract
Background: Opening wedge high-tibial osteotomy (OWHTO) is widely used for correcting mechanical axis deviations and offloading the medial compartment in unicompartmental osteoarthritis. However, lateral hinge fractures (LHFs) pose a significant complication. This study investigates protective measures to mitigate these fractures, guided by prior observations of mechanical stress impact on LHFs.
Purpose: The study aims to assess the effectiveness of different protective measures, specifically the use of varying sizes of Kirchner wires and drill holes, in reducing the incidence of LHFs during OWHTO. Study Design. The study employs a quantitative, comparative analysis using a finite element method (FEM) based on computed tomography (CT) scans.
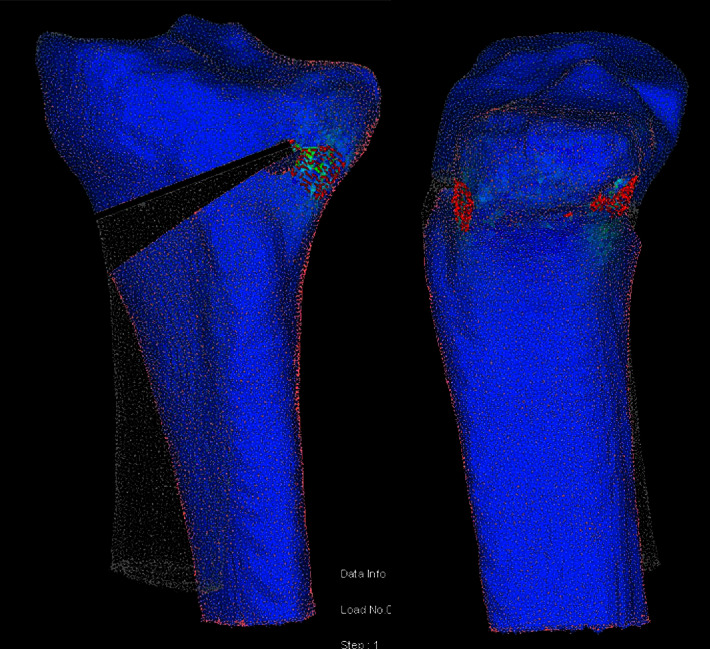
Methods: Using CT-based FEM, the study compares the impact of different sizes of K-wires (1.6 mm, 2.0 mm, and 2.5 mm) and drill holes (3.2 mm and 4.5 mm) on the mechanical stresses around the hinge area in OWHTO. The models were created from a CT scan of a healthy 33-year-old male, focusing on the force required to open the osteotomy gap and the incidence of cracked shell elements.
Results: The study found that thicker K-wires increased the force required to open the osteotomy gap, whereas larger apical holes decreased it. The 4.5 mm apical hole model demonstrated significantly fewer cracks compared to the 2.0 mm K-wire model, with no significant difference observed compared to the 2.5 mm K-wire model. Models using a 1.6 mm K-wire or a 3.2 mm drill hole did not significantly reduce cracks compared to the base model.
Conclusions: The findings suggest that a 4.5 mm drill hole may be more effective in reducing the risk of LHFs compared to thinner diameter K-wires or smaller apical holes. Both a 2.5 mm K-wire and a 4.5 mm drill hole reduce the number of cracked elements, but the 4.5 mm drill hole also significantly decreases the average and maximum principal stresses as well as the average tensile strength ratio at the hinge area. These findings may be important for surgical planning, particularly in cases requiring increased osteotomy distraction.
Copyright © 2024 Emre Özmen et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
The effect of lateral hinge fracture with hinge hole and protective K-wire for medial opening-wedge high tibial osteotomy by compression testing and finite element analysis.J Orthop Surg Res. 2025 Jun 17;20(1):598. doi: 10.1186/s13018-025-05993-9. J Orthop Surg Res. 2025. PMID: 40528197 Free PMC article.
-
Hinge location and apical drill holes in opening wedge high tibial osteotomy: A finite element analysis.J Orthop Res. 2021 Mar;39(3):628-636. doi: 10.1002/jor.24704. Epub 2020 May 7. J Orthop Res. 2021. PMID: 32352597
-
Quantitative analysis of protective Kirschner wire diameters in lateral opening wedge distal femoral osteotomy: A finite element study.Jt Dis Relat Surg. 2025 Jan 2;36(1):97-106. doi: 10.52312/jdrs.2025.1806. Epub 2024 Nov 5. Jt Dis Relat Surg. 2025. PMID: 39719906 Free PMC article.
-
Computed Tomography Detects Hinge Fractures After Medial Opening Wedge High Tibial Osteotomy: A Systematic Review.Arthroscopy. 2021 Apr;37(4):1337-1352. doi: 10.1016/j.arthro.2020.11.031. Epub 2020 Nov 23. Arthroscopy. 2021. PMID: 33242632
-
[Study on lateral hinge fracture during open wedge high tibial osteotomy].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2019 Jan 15;33(1):110-114. doi: 10.7507/1002-1892.201807049. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2019. PMID: 30644270 Free PMC article. Review. Chinese.
Cited by
-
Is it beneficial to use lateral protective crossing K-wires during medial open wedge high tibial osteotomy? A retrospective comparative study.J Orthop Surg Res. 2025 Feb 6;20(1):142. doi: 10.1186/s13018-025-05524-6. J Orthop Surg Res. 2025. PMID: 39910661 Free PMC article.
References
-
- Schubert M. F., Sidhu R., Getgood A. M., Sherman S. L. Failures of realignment osteotomy. Operative Techniques in Sports Medicine . 2020;28(1)150714
-
- Watanabe Y., Takenaka N., Kinugasa K., Matsushita T., Teramoto T. Intra‐and extra‐articular deformity of lower limb: tibial condylar valgus osteotomy (TCVO) and distal tibial oblique osteotomy (DTOO) for reconstruction of joint congruency. Advances in Orthopedics . 2019;2019 doi: 10.1155/2019/8605674.8605674 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
