

Inpatient Growth in Infants Requiring Pharmacologic Treatment for Neonatal Opioid Withdrawal Syndrome
- PMID: 39220832
- PMCID: PMC11366048
- DOI: 10.1155/2024/2212688
Inpatient Growth in Infants Requiring Pharmacologic Treatment for Neonatal Opioid Withdrawal Syndrome
Abstract
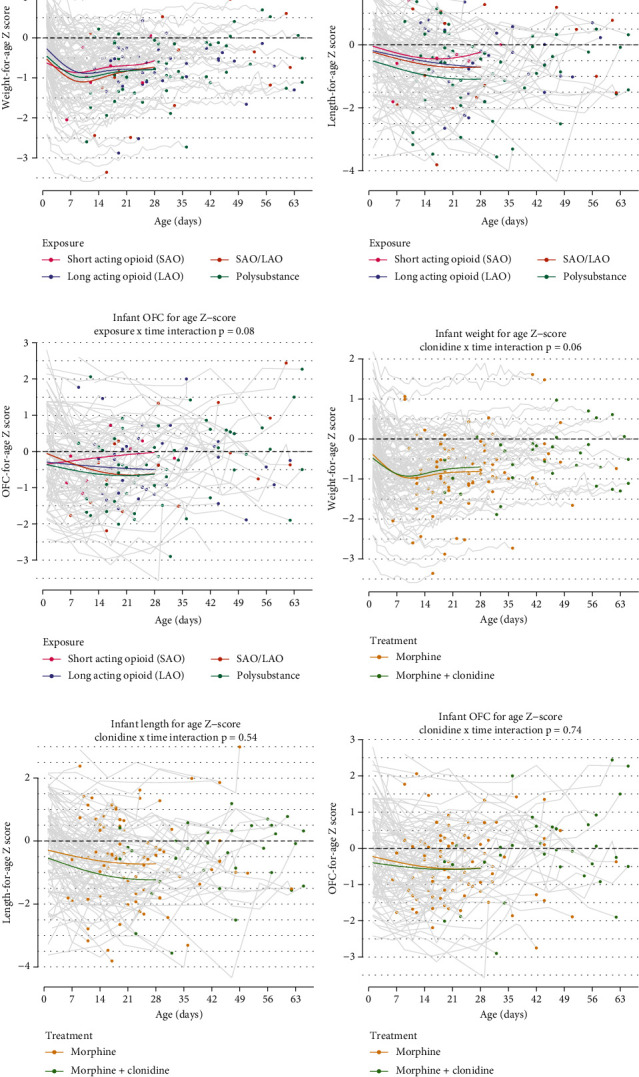
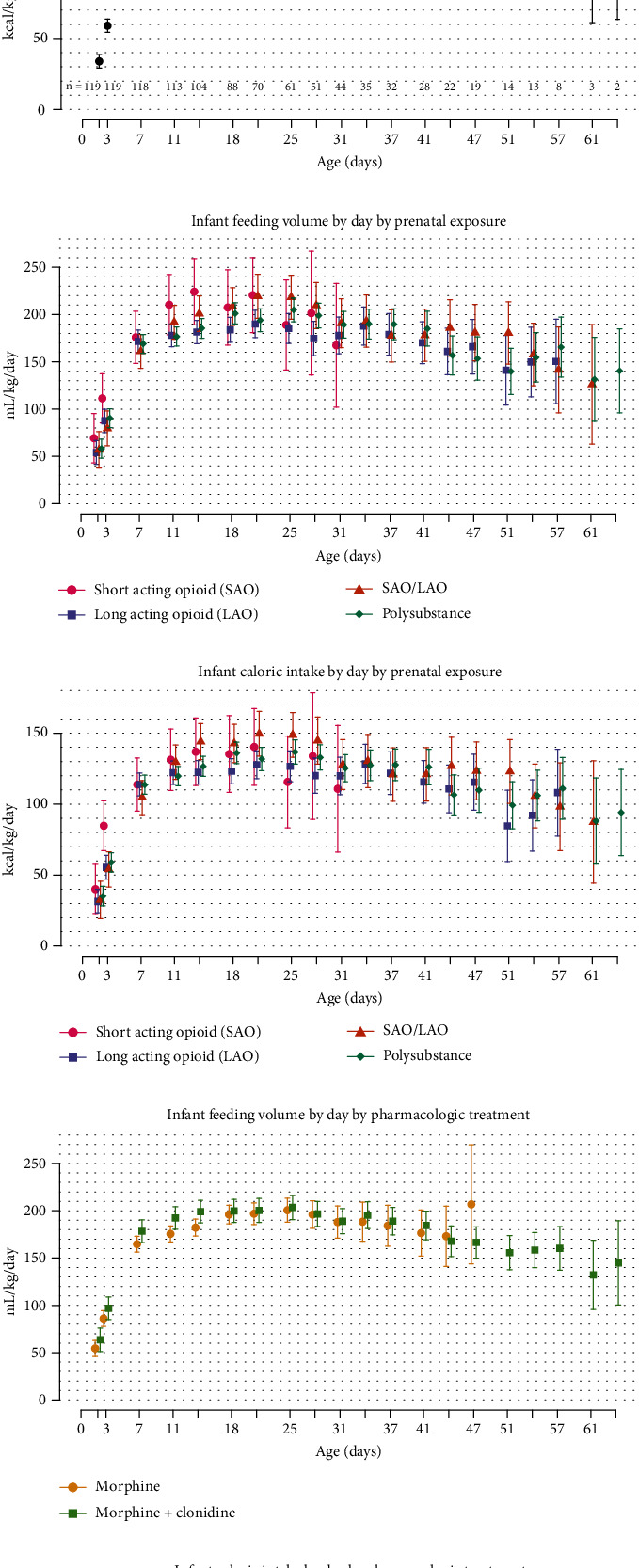
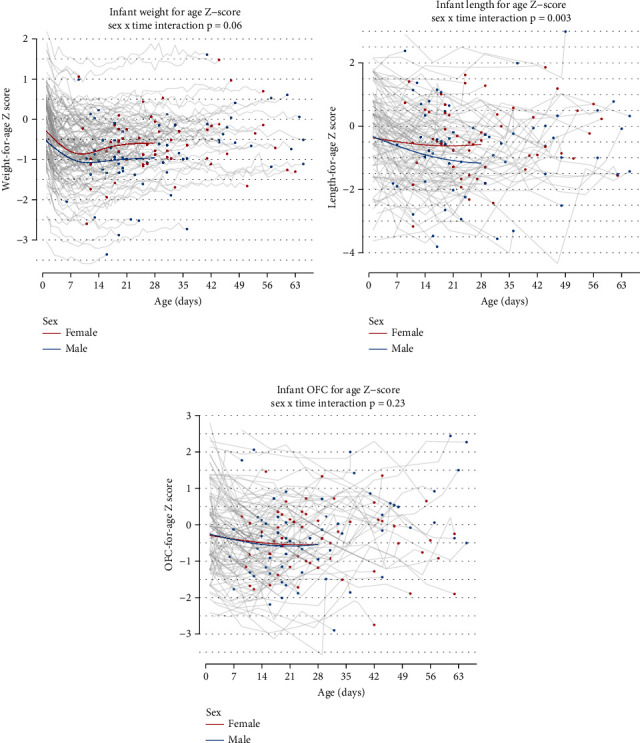
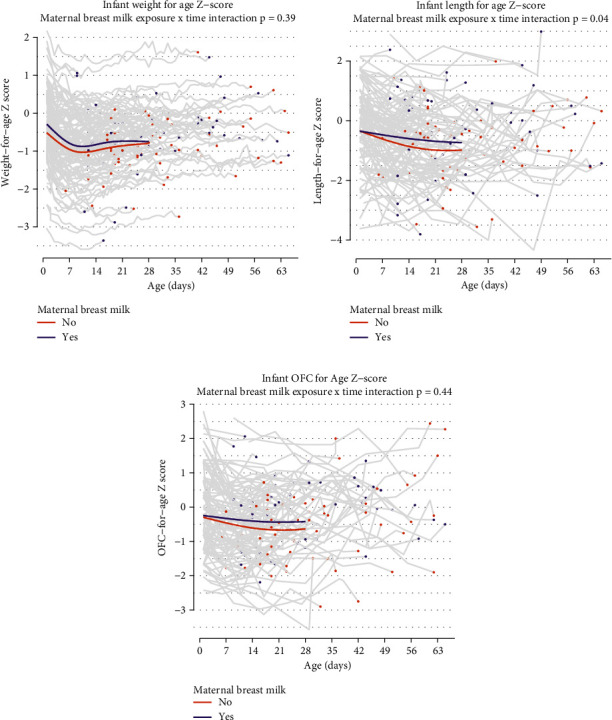
Aim: To assess inpatient growth parameter trajectories and to identify the type of opioid exposure and treatment characteristics influencing growth parameters of infants admitted to the newborn intensive care unit (NICU) for pharmacological treatment of neonatal opioid withdrawal syndrome (NOWS). Methods: Charts of term infants with NOWS admitted to NICU from 2012 to 2019, who received pharmacologic treatment, were reviewed. Intake (volume: mL/kg/day; calorie: kcal/kg/day) and growth parameter trajectories (weight, head circumference, and length) were analyzed based on the type of prenatal opioid exposure (short-acting opioids (SAOs), long-acting opioids (LAOs), and polysubstance), pharmacologic treatment, and sex. Growth measurement patterns over time were compared between groups using longitudinal mixed-effects models. Results: One hundred nineteen infants were included in the study with median birth weight Z-score of -0.19 at birth and decreased to a median of -0.72 at discharge. Exposure to SAO was associated with an increase in Z-scores nearing discharge across all growth parameters (Z-score for weight p = 0.03). Polysubstance exposure was associated with a decrease in Z-scores for length and head circumference throughout hospitalization. Infants with adjunct clonidine treatment had an increase in Z-score for weight trends. Male infants had a decrease in Z-scores for weight (male -0.96, female -0.59, interaction p = 0.06) and length (male -1.17, female -0.57, interaction p = 0.003) at Day 28. Despite the difference in growth trajectories, intake in terms of amount (mL/kg/day) and calorie intake (kcal/kg/day) was similar based on prenatal exposure, treatment, and sex. Conclusion: Infants with NOWS requiring pharmacologic treatment have a decrease in Z-scores for weight, length, and head circumference at birth and at hospital discharge. Infants with prenatal polysubstance exposure were at particular risk for poorer inpatient growth relative to infants exposed to SAO and LAO, indicated by lower Z-scores for length and occipital frontal circumference (OFC).
Keywords: Z-score; growth trajectories; head circumference; length; neonatal opioid withdrawal syndrome; opioids; weight.
Copyright © 2024 Ashajyothi M. Siddappa et al.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Patrick S. W., Schumacher R. E., Benneyworth B. D., Krans E. E., McAllister J. M., Davis M. M. Neonatal abstinence syndrome and associated health care expenditures: United States, 2000-2009. Journal of the American Medical Association . 2012;307(18):1934–1940. doi: 10.1001/jama.2012.3951. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
