

Fascial Plane Blocks With Glucocorticoids or Liposomal Bupivacaine Versus Local Infiltration for Laparoscopic Non-donor Nephrectomy: A Propensity Score-Weighted Study
- PMID: 39221354
- PMCID: PMC11366221
- DOI: 10.7759/cureus.66005
Fascial Plane Blocks With Glucocorticoids or Liposomal Bupivacaine Versus Local Infiltration for Laparoscopic Non-donor Nephrectomy: A Propensity Score-Weighted Study
Abstract
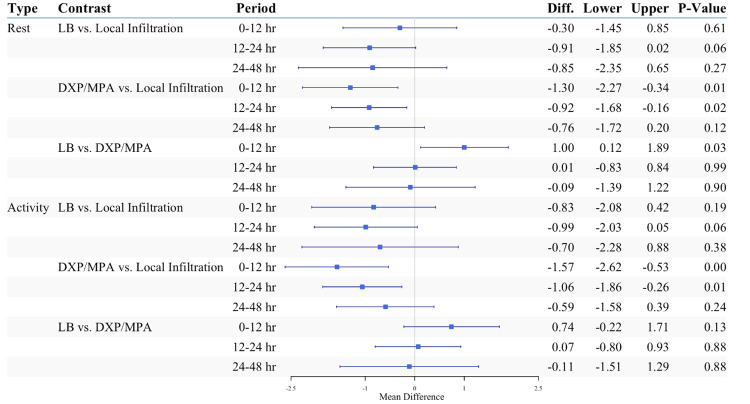
Study objective The purpose of this study is to investigate the analgesic efficacy of ultrasound-guided fascial plane blocks (FPBs) versus local infiltration in patients undergoing laparoscopic non-donor nephrectomy. This study specifically compares the efficacy of FPBs with liposomal bupivacaine (LB) versus FPBs with dexamethasone sodium phosphate (DXP) and methylprednisolone acetate (MPA) versus surgical site local anesthetic infiltration without FPBs. Design This is a retrospective cohort study conducted over a five-year period (January 2018-December 2022). Setting The study was conducted in a tertiary care, academic, multi-hospital healthcare system. Participants Patients who underwent elective radical or partial laparoscopic non-donor nephrectomy were included in the study. Intervention Patients either received preoperative FPBs without intraoperative surgical site local anesthetic infiltration or received surgical site local anesthetic infiltration without FPBs (n = 141) at participating hospitals. Measurements The primary endpoint of this study was postoperative opioid use, measured as oral milligram morphine equivalents (MME). Secondary endpoints included postoperative pain scores, length of hospital stays, and significant adverse events within 30 days. The impact of medications utilized in FPBs was determined by univariate and multivariable analyses with covariates balancing propensity score weighting. Main results Patients undergoing non-donor laparoscopic radical or partial nephrectomy who received FPBs with bupivacaine or ropivacaine plus glucocorticoids DXP and MPA were more likely to be opioid-free 24-48 hours postoperatively compared to those who received FPBs with LB or surgical site local anesthetic infiltration without FPBs (40.5% vs. 30% vs. 13.9%, respectively; p = 0.017). Patients who received FPBs with glucocorticoids also reported the lowest pain scores at rest and with activity 0-12 hours postoperatively as compared to patients who received LB or local infiltration (p = 0.006 and p = 0.014, respectively). Additionally, patients who received FPBs with glucocorticoids received over 30% fewer opioids during the first 48 hours postoperatively compared to patients who received surgical site local anesthetic infiltration alone (30 MME vs. 44 MME, respectively). However, there was no significant difference in total opioid use during the first 48 hours postoperatively between patients who received FPBs with bupivacaine plus glucocorticoids and those who received FPBs with bupivacaine plus LB (mean ratio: 0.91, (95% CI: 0.05 ~ 15.97); p = 0.948). There was also no difference in the length of hospital stays or rate of adverse events between the groups. Conclusion Perioperative FPBs for non-donor laparoscopic nephrectomy using glucocorticoids as an adjuvant to long-acting local anesthetics may decrease postoperative opioid use and reduce pain scores as compared to FPBs with LB or surgical site local anesthetic infiltration. Bupivacaine or ropivacaine combined with DXP and MPA is a safe and effective alternative to LB for FPBs in laparoscopic nephrectomy.
Keywords: dexamethasone; fascial plane block; liposomal bupivacaine; methylprednisolone acetate; nephrectomy.
Copyright © 2024, Sobhani et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Yale School of Medicine Institutional Review Board (IRB) issued approval (2000029282). Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures



References
-
- Minimally invasive vs open nephrectomy in the modern era: does approach matter? Golombos DM, Chughtai B, Trinh QD, et al. World J Urol. 2017;35:1557–1568. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous