

Lesion-Level Effects of LDL-C-Lowering Therapy in Patients With Acute Myocardial Infarction: A Post Hoc Analysis of the PACMAN-AMI Trial
- PMID: 39221516
- PMCID: PMC11369785
- DOI: 10.1001/jamacardio.2024.3200
Lesion-Level Effects of LDL-C-Lowering Therapy in Patients With Acute Myocardial Infarction: A Post Hoc Analysis of the PACMAN-AMI Trial
Abstract
Importance: Previous studies investigated atherosclerotic changes induced by lipid-lowering therapy in extensive coronary segments irrespective of baseline disease burden (a vessel-level approach).
Objective: To investigate the effects of lipid-lowering therapy on coronary lesions with advanced atherosclerotic plaque features and presumably higher risk for future events.
Design, setting, and participants: The PACMAN-AMI randomized clinical trial (enrollment: May 2017 to October 2020; final follow-up: October 2021) randomized patients with acute myocardial infarction to receive alirocumab or placebo in addition to high-intensity statin therapy. In this post hoc lesion-level analysis, nonculprit lesions were identified as segments with plaque burden 40% or greater defined by intravascular ultrasound (IVUS). IVUS, near-infrared spectroscopy, and optical coherence tomography images at baseline and the 52-week follow-up were manually matched by readers blinded to treatment allocation. Data for this study were analyzed from October 2022 to November 2023.
Interventions: Alirocumab or placebo in addition to high-intensity statin therapy.
Main outcomes and measures: Lesion-level imaging outcome measures, including high-risk plaque characteristics and phenotypes.
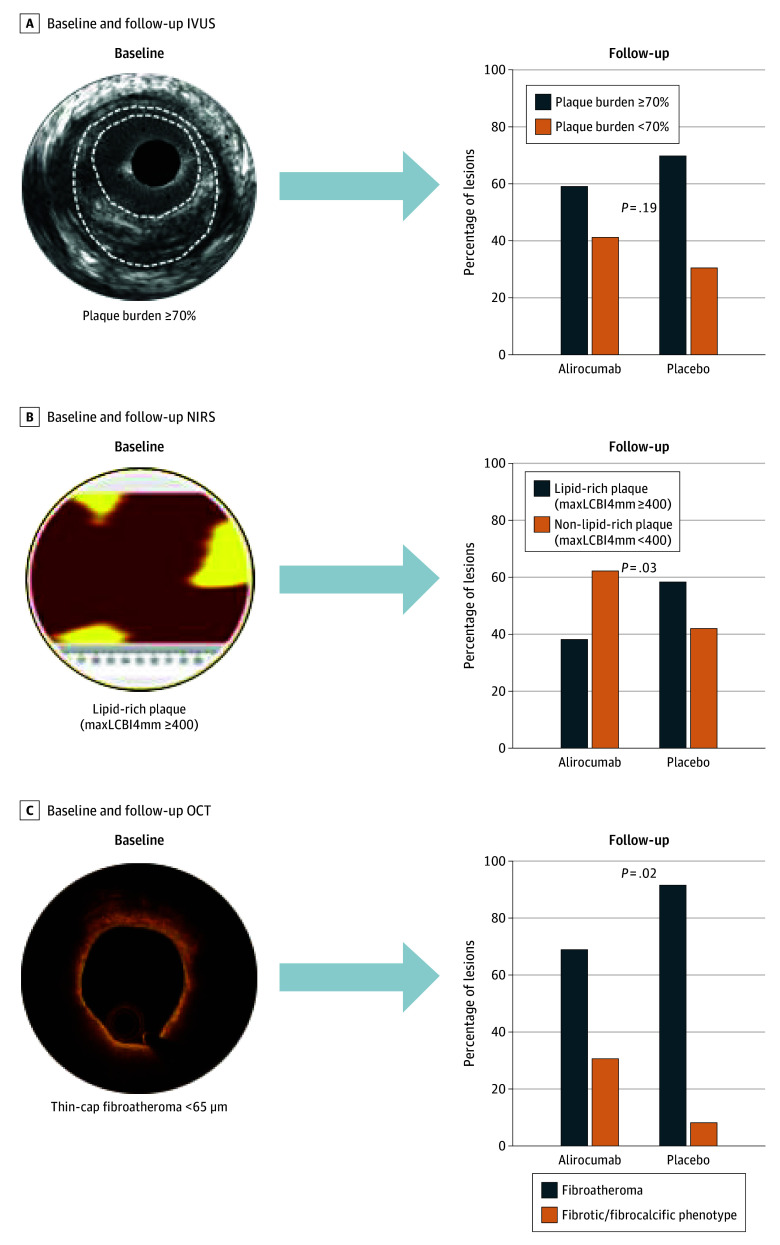
Results: Of the 245 patients in whom lesions were found, 118 were in the alirocumab group (mean [SD] age, 58.2 [10.0] years; 101 [85.6%] male and 17 [14.4%] female) and 127 in the placebo group (mean [SD] age, 57.7 [8.8] years; 104 [81.9%] male and 23 [18.1%] female). Overall, 591 lesions were included: 287 lesions (118 patients, 214 vessels) in the alirocumab group and 304 lesions (127 patients, 239 vessels) in the placebo group. Lesion-level mean change in percent atheroma volume (PAV) was -4.86% with alirocumab vs -2.78% with placebo (difference, -2.02; 95% CI, -3.00 to -1.05; P < .001). At the minimum lumen area (MLA) site, mean change in PAV was -10.14% with alirocumab vs -6.70% with placebo (difference, -3.36; 95% CI, -4.98 to -1.75; P < .001). MLA increased by 0.15 mm2 with alirocumab and decreased by 0.07 mm2 with placebo (difference, 0.21; 95% CI, 0.01 to 0.41; P = .04). Among 122 lipid-rich lesions, 34 of 55 (61.8%) in the alirocumab arm and 27 of 67 (41.8%) in the placebo arm showed a less lipid-rich plaque phenotype at follow-up (P = .03). Among 63 lesions with thin-cap fibroatheroma at baseline, 8 of 26 (30.8%) in the alirocumab arm and 3 of 37 (8.1%) in the placebo arm showed a fibrous/fibrocalcific plaque phenotype at follow-up (P = .02).
Conclusions and relevance: At the lesion level, very intensive lipid-lowering therapy induced substantially greater PAV regression than described in previous vessel-level analyses. Compared with statin therapy alone, alirocumab treatment was associated with greater enlargement of the lesion MLA and more frequent transition of presumably high-risk plaque phenotypes into more stable, less lipid-rich plaque phenotypes.
Trial registration: ClinicalTrials.gov Identifier: NCT03067844.
Conflict of interest statement
Figures


Comment on
-
What We Have Learned About Reducing Low-Density Lipoprotein Cholesterol and Coronary Plaques.JAMA Cardiol. 2024 Dec 1;9(12):1092-1093. doi: 10.1001/jamacardio.2024.3213. JAMA Cardiol. 2024. PMID: 39221517 No abstract available.
References
-
- Erlinge D, Maehara A, Ben-Yehuda O, et al. ; PROSPECT II Investigators . Identification of vulnerable plaques and patients by intracoronary near-infrared spectroscopy and ultrasound (PROSPECT II): a prospective natural history study. Lancet. 2021;397(10278):985-995. doi: 10.1016/S0140-6736(21)00249-X - DOI - PubMed
-
- Waksman R, Di Mario C, Torguson R, et al. ; LRP Investigators . Identification of patients and plaques vulnerable to future coronary events with near-infrared spectroscopy intravascular ultrasound imaging: a prospective, cohort study. Lancet. 2019;394(10209):1629-1637. doi: 10.1016/S0140-6736(19)31794-5 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
