

Epidemiology of acute hypoxaemic respiratory failure in Australian and New Zealand intensive care units during 2005-2022. A binational, registry-based study
- PMID: 39222135
- PMCID: PMC11541379
- DOI: 10.1007/s00134-024-07609-y
Epidemiology of acute hypoxaemic respiratory failure in Australian and New Zealand intensive care units during 2005-2022. A binational, registry-based study
Abstract
Purpose: Acute hypoxaemic respiratory failure (AHRF) is a common reason for intensive care unit (ICU) admission. However, patient characteristics, outcomes, and trends over time are unclear. We describe the epidemiology and outcomes of patients with AHRF over time.
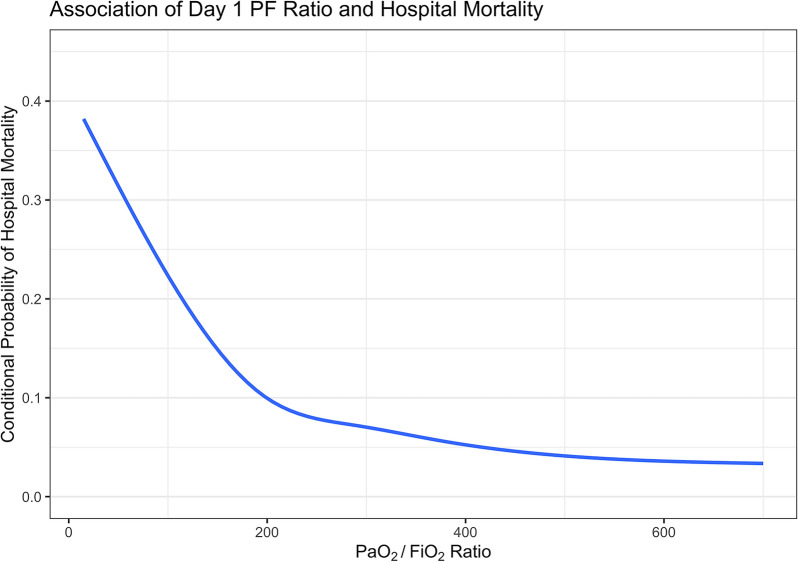
Methods: In this binational, registry-based study from 2005 to 2022, we included all adults admitted to an Australian or New Zealand ICU with an arterial blood gas within the first 24 h of ICU stay. AHRF was defined as a partial pressure of oxygen/inspired oxygen ratio (PaO2/FiO2) ≤ 300. The primary outcome was adjusted in-hospital mortality, categorised based on PaO2/FiO2 (mild: 200-300, moderate: 100-200, and severe < 100, and non-linearly). We investigated how adjusted mortality evolved based on temporal trends (by year of admission), sex, age, admission diagnosis and the receipt of mechanical ventilation.
Results: Of 1,560,221 patients, 826,106 (52.9%) were admitted with or developed AHRF within the first 24 h of ICU stay. Of these 826,106 patients, 51.4% had mild, 39.3% had moderate, and 9.3% had severe AHRF. Compared to patients without AHRF (5.3%), patients with mild (8%), moderate (14.2%) and severe (29.9%) AHRF had higher in-hospital mortality rates. As PaO2/FiO2 ratio decreased, adjusted in-hospital mortality progressively increased, particularly below an inflection point at a PaO2/FiO2 ratio of 200. The adjusted in-hospital mortality for all patients decreased over time (13.3% in 2005 to 8.2% in 2022), and this trend was similar in patients with and without AHRF.
Conclusion: The healthcare burden due to AHRF may be larger than expected, and mortality rates remain high in severe AHRF. Although mortality has decreased over time, this may reflect improvements in ICU care in general, rather than specifically in AHRF. More research is required to earlier identify AHRF and stratify these patients at risk of deterioration early, and to validate our findings.
Keywords: AHRF; Acute hypoxaemic respiratory failure; Hypoxaemia; Intensive care; Mortality; PaO2/FiO2; Respiratory failure.
© 2024. The Author(s).
Conflict of interest statement
RRL receives research support from the Clinician Scientist Development Unit, Yong Loo Lin School of Medicine, National University of Singapore. AB is a recipient of the National Health and Medical Research Council Emerging Leader Fellowship (201110). DP is the chairman of the ANZICS Centre for Outcomes and Resources Evaluation Clinical Quality Registry and is the vice-president and board member of ANZICS. All other authors declare no competing interests. KS acknowledges Metro Health. No other conflicts of interest for other authors.
Figures


References
-
- Villar J, Blanco J, Añón JM, Santos-Bouza A, Blanch L, Ambrós A, Gandía F, Carriedo D, Mosteiro F, Basaldúa S, Fernández RL, Kacmarek RM (2011) The ALIEN study: incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Med 37:1932–1941 - PubMed
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS (2012) Acute respiratory distress syndrome: the Berlin Definition. JAMA 307:2526–2533 - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G et al (2016) Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 315:788–800 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
