

Teriparatide in postmenopausal osteoporosis: uncovering novel insights into efficacy and safety compared to other treatments - a systematic review and meta-analysis
- PMID: 39222329
- PMCID: PMC11457814
- DOI: 10.1530/EOR-23-0205
Teriparatide in postmenopausal osteoporosis: uncovering novel insights into efficacy and safety compared to other treatments - a systematic review and meta-analysis
Abstract
Objective: The aim of the study was to evaluate the efficacy and safety of teriparatide compared to other treatments for postmenopausal osteoporosis.
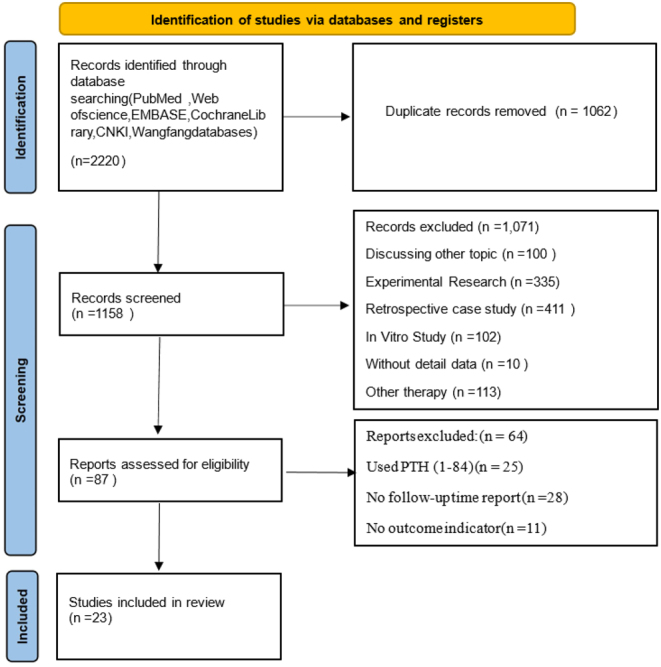
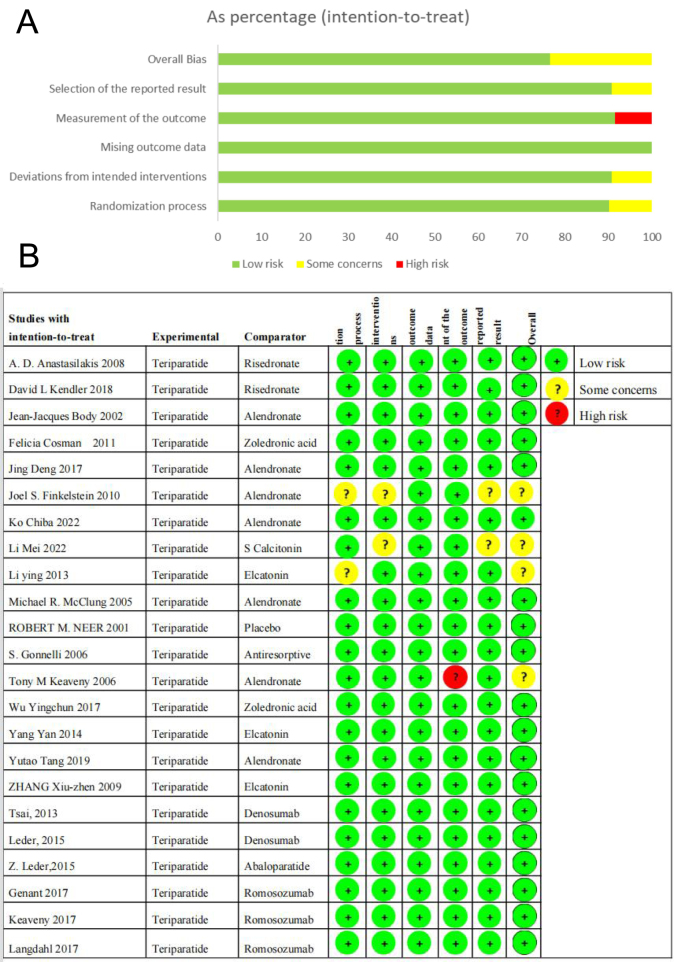
Methods: A review of studies from 2000 to January 2023 analyzed randomized controlled trials on postmenopausal women treated with teriparatide (PTH 1-34), comparing it to placebo or other osteoporosis treatments. The analysis focused on bone mineral density (BMD), bone turnover markers, and clinical outcomes, employing Review Manager 5.4.1 and the RoB 2 tool for bias assessment.
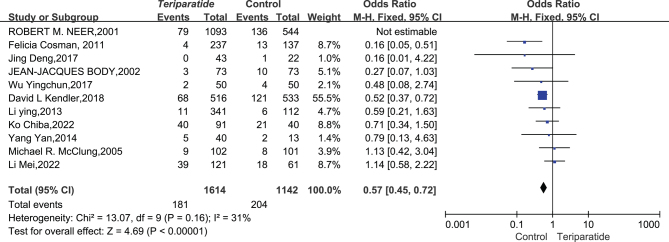
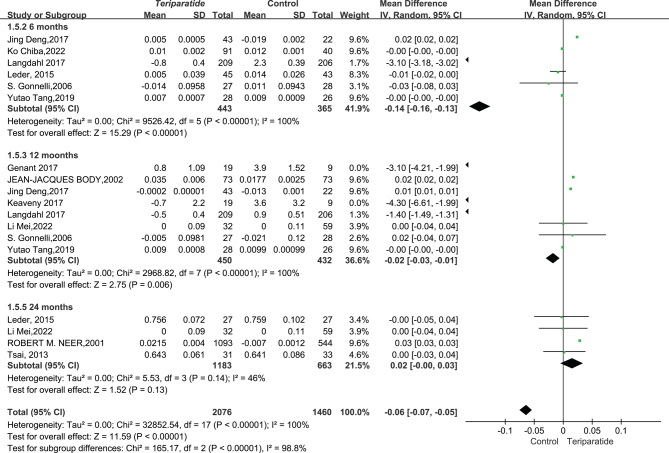
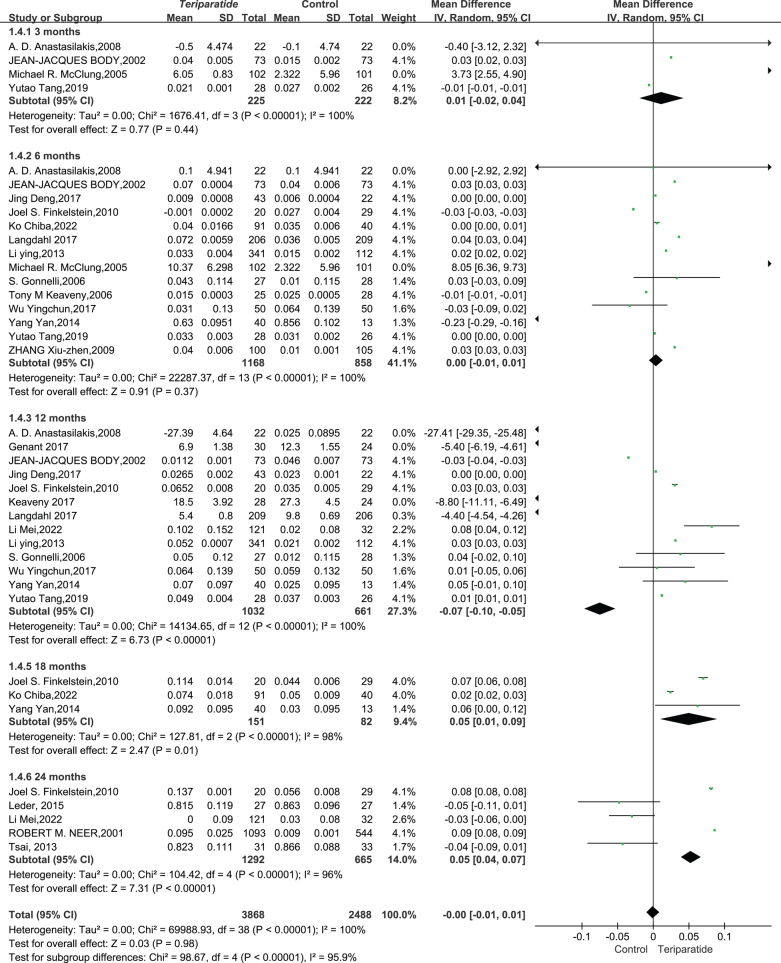
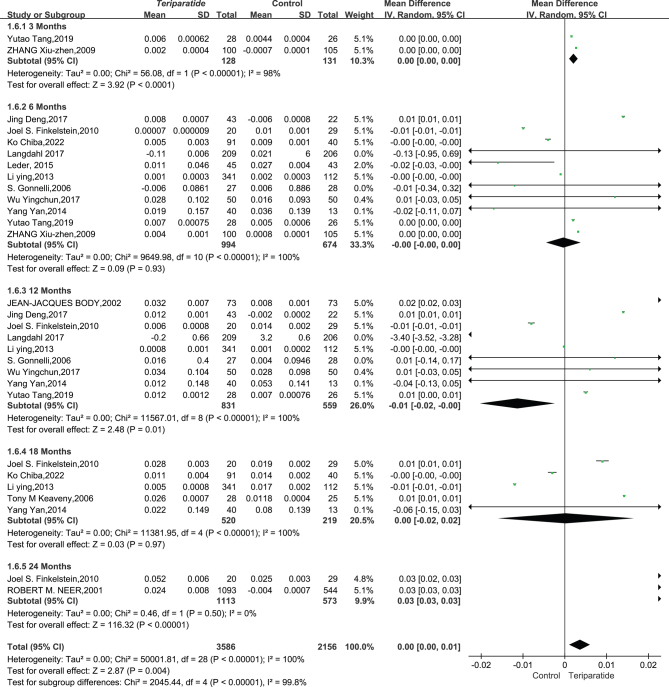
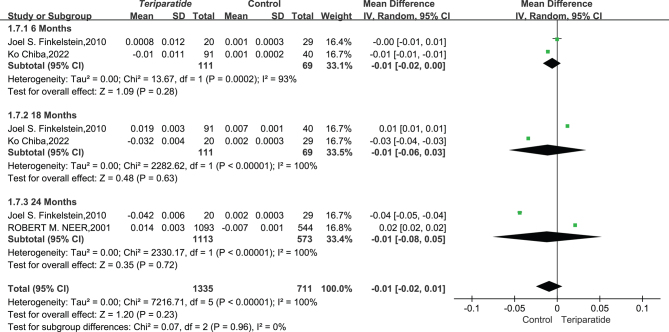
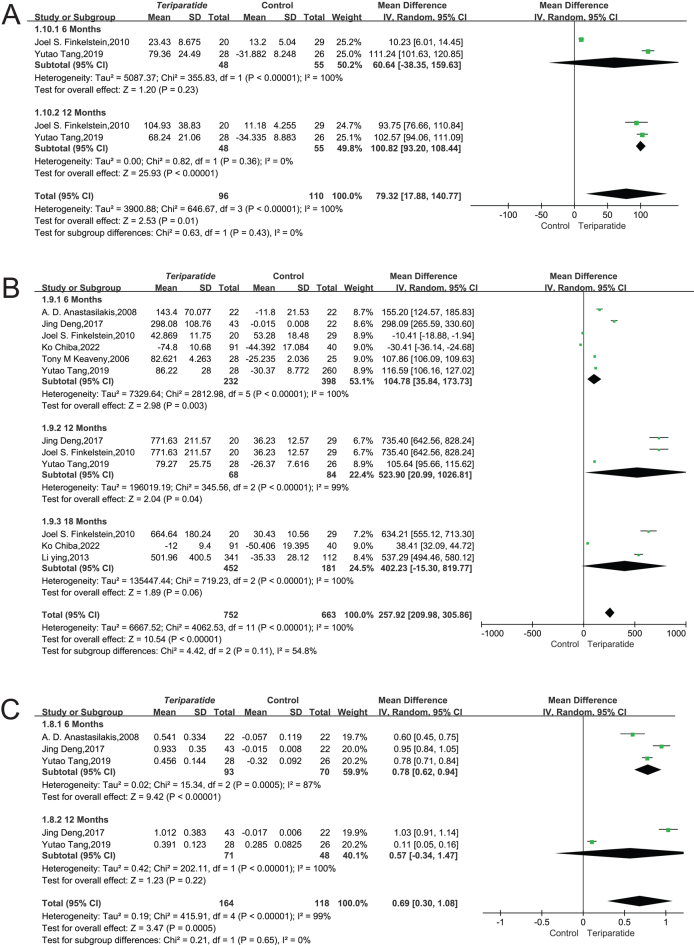
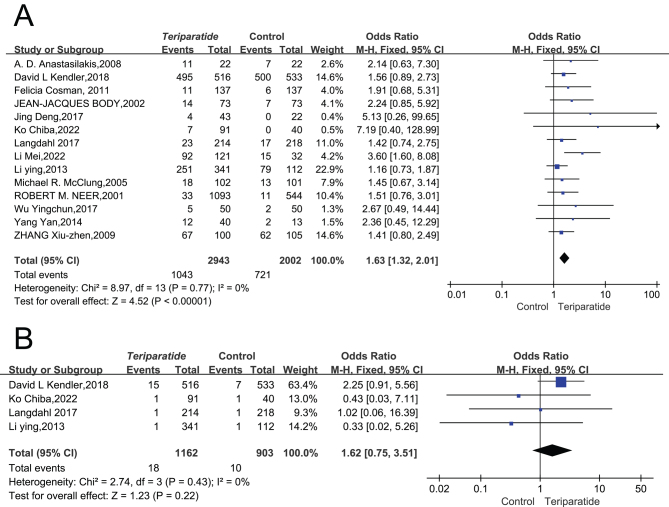
Results: Our analysis of 23 randomized controlled trials (RCTs) found that PTH (134) treatment significantly increased lumbar spine BMD (mean difference (MD) = 0.02, 95% CI: 0.01-0.03) and femoral neck BMD (MD = 0.01, 95% CI: 0.00-0.01). However, there were no significant changes in total hip and radial bone BMD among the 3536 and 2046 participants, respectively. We also found that PTH (1-34) increased P1NP in a larger cohort (n = 1415) when compared to osteocalcin (n = 206). Although the risk of adverse events increased (relative risk (RR) = 1.65, 95% CI: 1.32-2.07), the incidence of fractures decreased significantly (RR = 0.57, 95% CI: 0.45-0.072), with no significant difference observed in mortality rates between treatment and control groups.
Conclusion: Teriparatide improves lumbar spine and femoral neck BMD in postmenopausal women. Particularly notable is the novel finding regarding its effect on radius BMD, an area less explored in previous research. Despite an uptick in adverse events, the marked decrease in fracture incidence confirms its clinical utility for high-risk osteoporosis patients, highlighting the necessity for ongoing investigations into its full skeletal effects.
Keywords: fractures; parathyroid hormone; postmenopausal osteoporosis; systematic review; teriparatide.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the study reported.
Figures
References
-
- Report of a WHO Study Group Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. World Health Organization Technical Report Series; 19948431–29. - PubMed
LinkOut - more resources
Full Text Sources
