

Association Between False-Positive Results and Return to Screening Mammography in the Breast Cancer Surveillance Consortium Cohort
- PMID: 39222505
- PMCID: PMC11970968
- DOI: 10.7326/M24-0123
Association Between False-Positive Results and Return to Screening Mammography in the Breast Cancer Surveillance Consortium Cohort
Abstract
Background: False-positive results on screening mammography may affect women's willingness to return for future screening.
Objective: To evaluate the association between screening mammography results and the probability of subsequent screening.
Design: Cohort study.
Setting: 177 facilities participating in the Breast Cancer Surveillance Consortium (BCSC).
Patients: 3 529 825 screening mammograms (3 184 482 true negatives and 345 343 false positives) performed from 2005 to 2017 among 1 053 672 women aged 40 to 73 years without a breast cancer diagnosis.
Measurements: Mammography results (true-negative result or false-positive recall with a recommendation for immediate additional imaging only, short-interval follow-up, or biopsy) from 1 or 2 screening mammograms. Absolute differences in the probability of returning for screening within 9 to 30 months of false-positive versus true-negative screening results were estimated, adjusting for race, ethnicity, age, time since last mammogram, BCSC registry, and clustering within women and facilities.
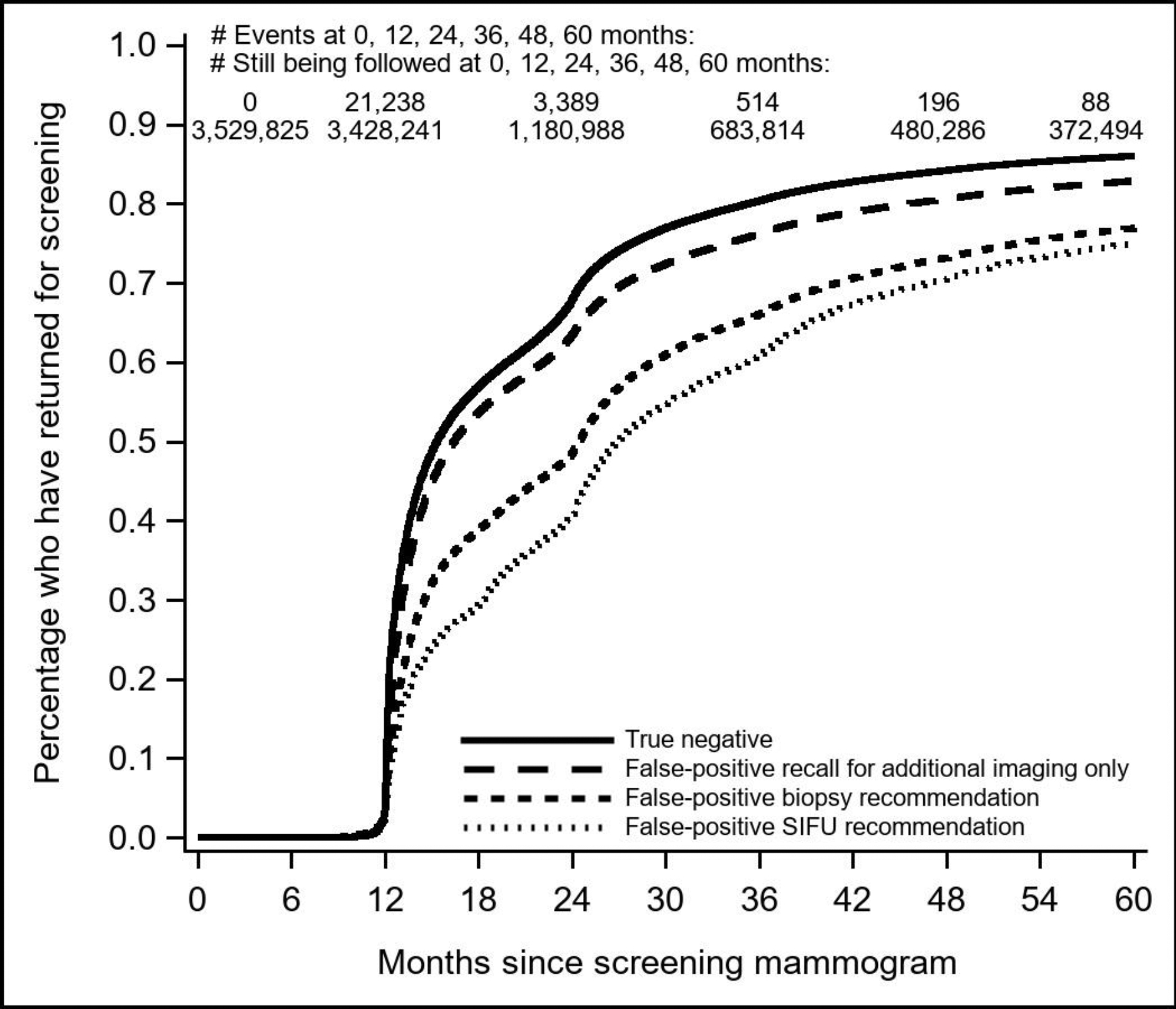
Results: Women were more likely to return after a true-negative result (76.9% [95% CI, 75.1% to 78.6%]) than after a false-positive recall for additional imaging only (adjusted absolute difference, -1.9 percentage points [CI, -3.1 to -0.7 percentage points]), short-interval follow-up (-15.9 percentage points [CI, -19.7 to -12.0 percentage points]), or biopsy (-10.0 percentage points [CI, -14.2 to -5.9 percentage points]). Asian and Hispanic/Latinx women had the largest decreases in the probability of returning after a false positive with a recommendation for short-interval follow-up (-20 to -25 percentage points) or biopsy (-13 to -14 percentage points) versus a true negative. Among women with 2 screening mammograms within 5 years, a false-positive result on the second was associated with a decreased probability of returning for a third regardless of the first screening result.
Limitation: Women could receive care at non-BCSC facilities.
Conclusion: Women were less likely to return to screening after false-positive mammography results, especially with recommendations for short-interval follow-up or biopsy, raising concerns about continued participation in routine screening among these women at increased breast cancer risk.
Primary funding source: National Cancer Institute.
Conflict of interest statement
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical