

The Efficacy of Modified Ilizarov Distraction-Tension Device on Limb Wound Difficult to Cover with Skin Flaps
- PMID: 39223103
- PMCID: PMC11572560
- DOI: 10.1111/os.14217
The Efficacy of Modified Ilizarov Distraction-Tension Device on Limb Wound Difficult to Cover with Skin Flaps
Abstract
Introduction: Closure of complex limb wounds poses challenges and requires innovative approaches. This research aimed to evaluate the effectiveness of a modified distraction-tension device using Ilizarov external fixation for wound closure in challenging cases.
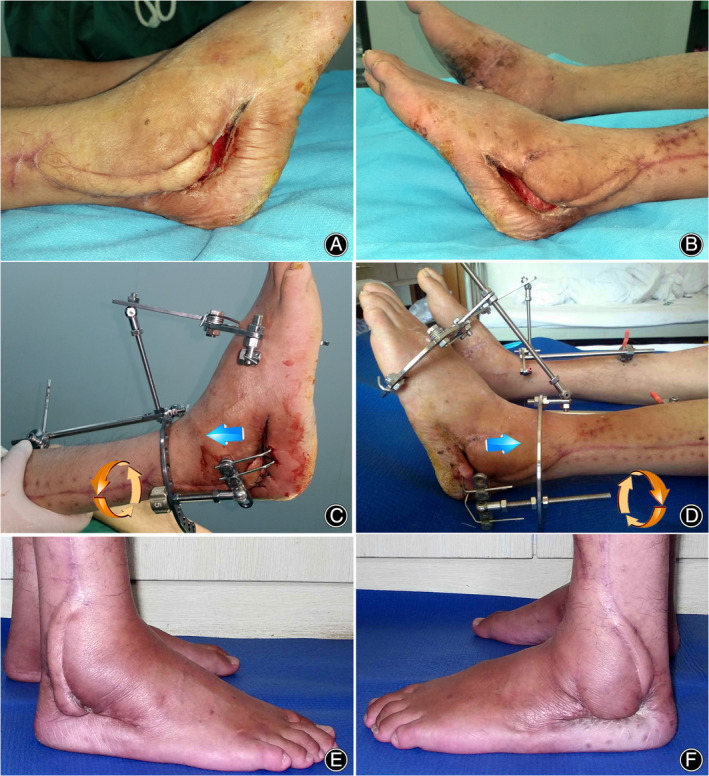
Methods: A retrospective analysis was conducted on 43 patients with extremity wounds that were difficult to cover with skin flaps between January 2019 and December 2022. Tension-relieving traction was applied using the Ilizarovexternal fixator apparatus, tailored to individual wound characteristics. Three types of wire-pin connections were used in this study. The distraction begins on the third postoperative day, with a speed of 0.5mm/d. Clinical wound healing scores were evaluated at 5 and 30 days postoperatively. Complications were documented following the Paley classification system.
Results: Traction using modified Ilizarovexternal fixation promoted a significant reduction in wound size. The mean traction period was 11.2 ± 7.3 days, and the mean healing duration was 17.0 ± 3.7 days. The clinical wound healing score improved from 3.7 ± 2.9 at 5 days to 1.7 ± 0.7 at 30 days postoperatively (p < 0.05). Complications were minimal, with no significant obstacles or sequelae observed. Direct closure healing was achieved in 21 cases, skin graft healing in 13 cases, and suture healing in 9 cases. No recurrences were reported. Using Paley's classified complications, there were 17 problems, 9 obstacles, and 0 sequelae.
Conclusion: The Ilizarov tension-relieving traction shows promise in facilitating wound closure that is challenging to manage with skin flaps. The modified three types of pin-skin connection configuration could satisfy various types of wound closure.
Keywords: Complex Limb Wounds; Ilizarov Tension‐Relieving Traction; Modified Ilizarov external fixation; Skin Flaps; Wound Closure Effectiveness.
© 2024 The Author(s). Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
All authors have no competing interests.
Figures



References
-
- Alga A, Haweizy R, Bashaireh K, Wong S, Lundgren KC, von Schreeb J, et al. Negative pressure wound therapy versus standard treatment in patients with acute conflict‐related extremity wounds: a pragmatic, multisite, randomised controlled trial. Lancet Glob Health. 2020;8:e423–e429. 10.1016/S2214-109X(19)30547-9 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
