

SGLT2 inhibition mitigates transition from acute kidney injury to chronic kidney disease by suppressing ferroptosis
- PMID: 39223189
- PMCID: PMC11369184
- DOI: 10.1038/s41598-024-71416-0
SGLT2 inhibition mitigates transition from acute kidney injury to chronic kidney disease by suppressing ferroptosis
Abstract
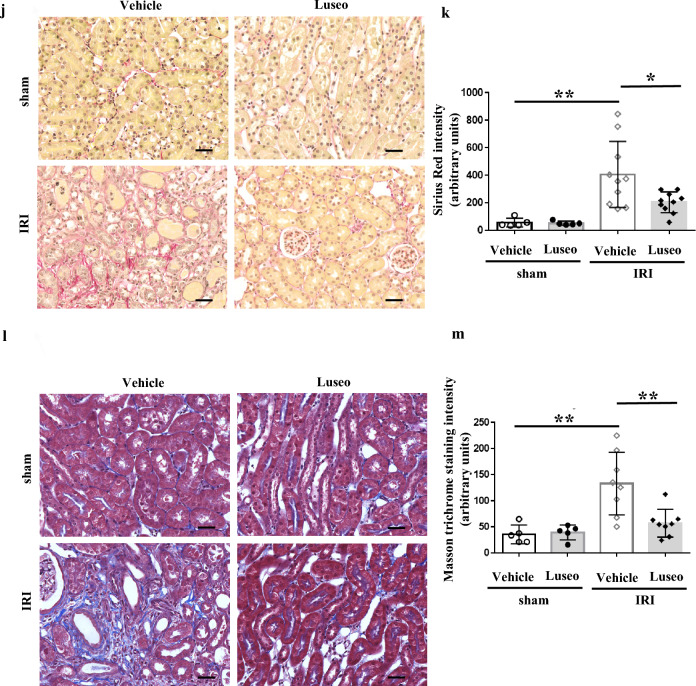
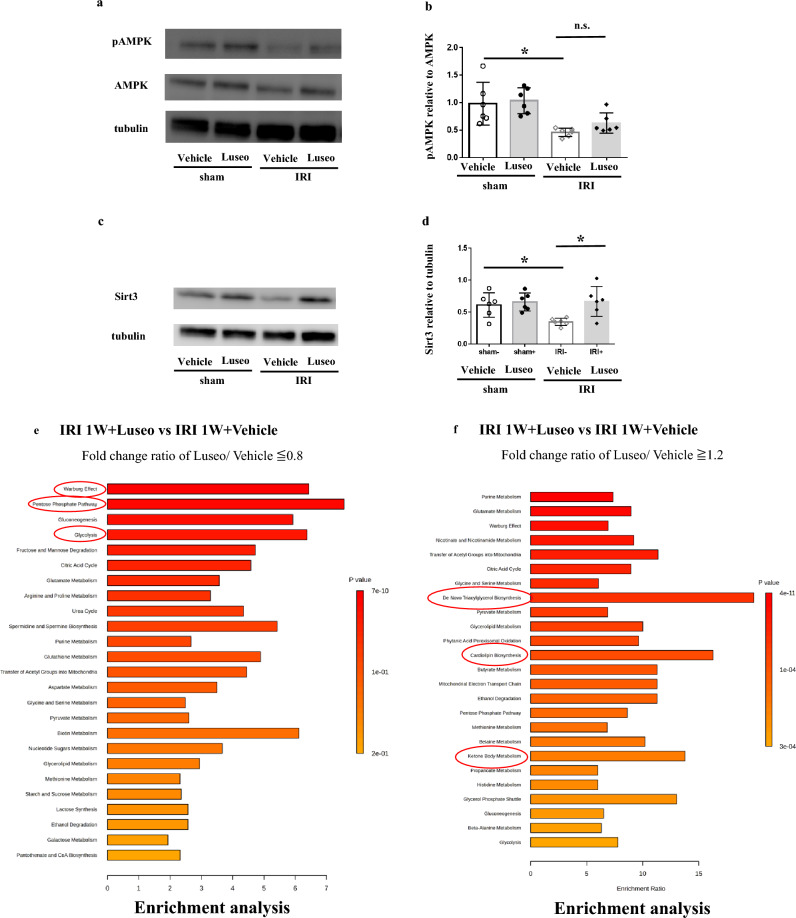
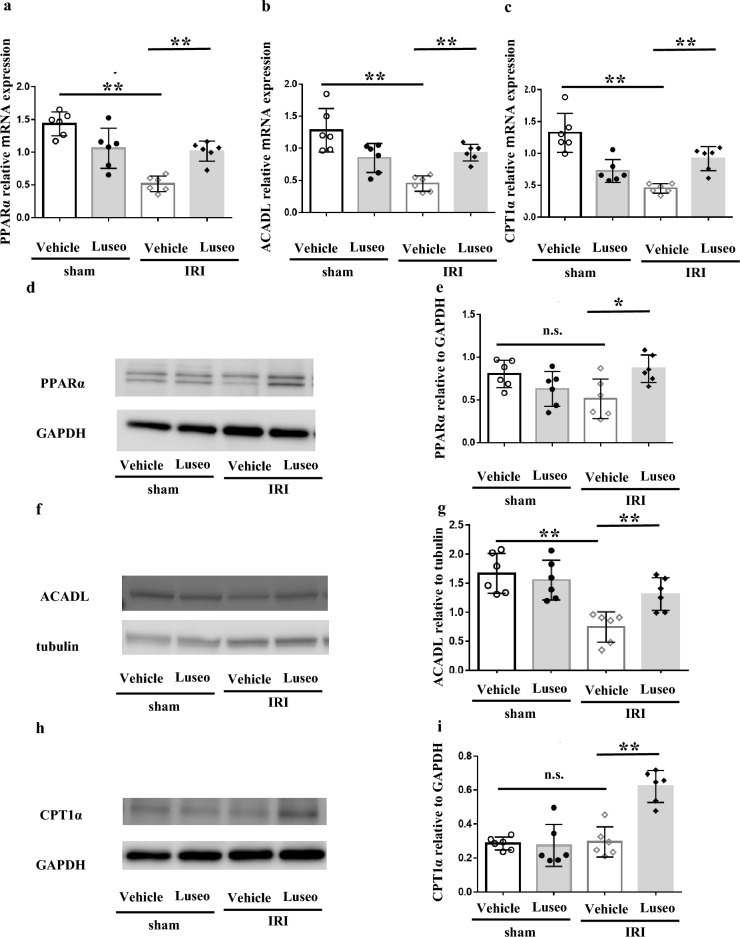
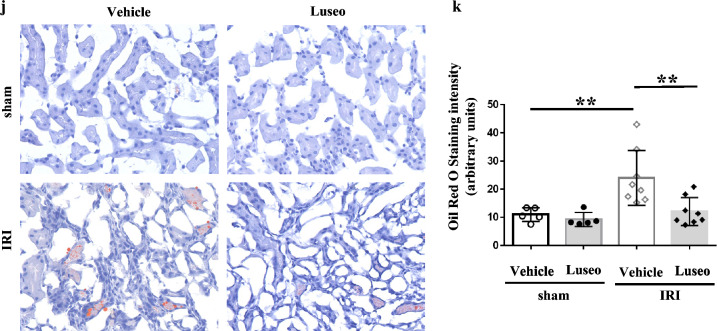
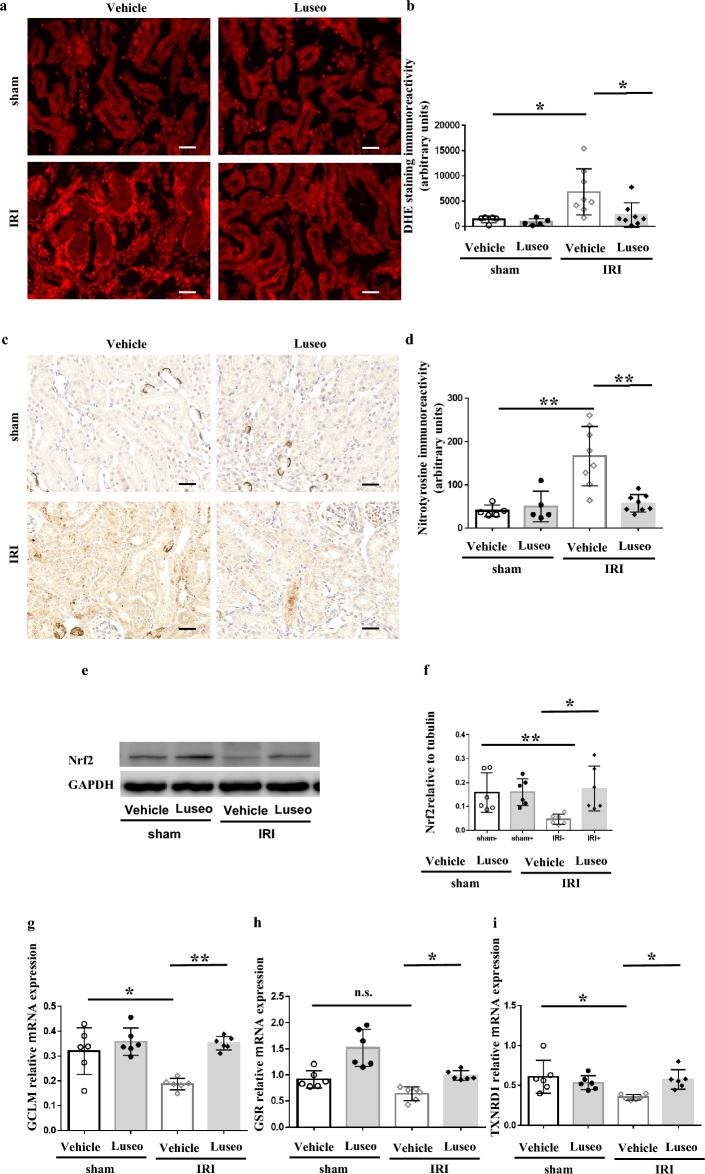
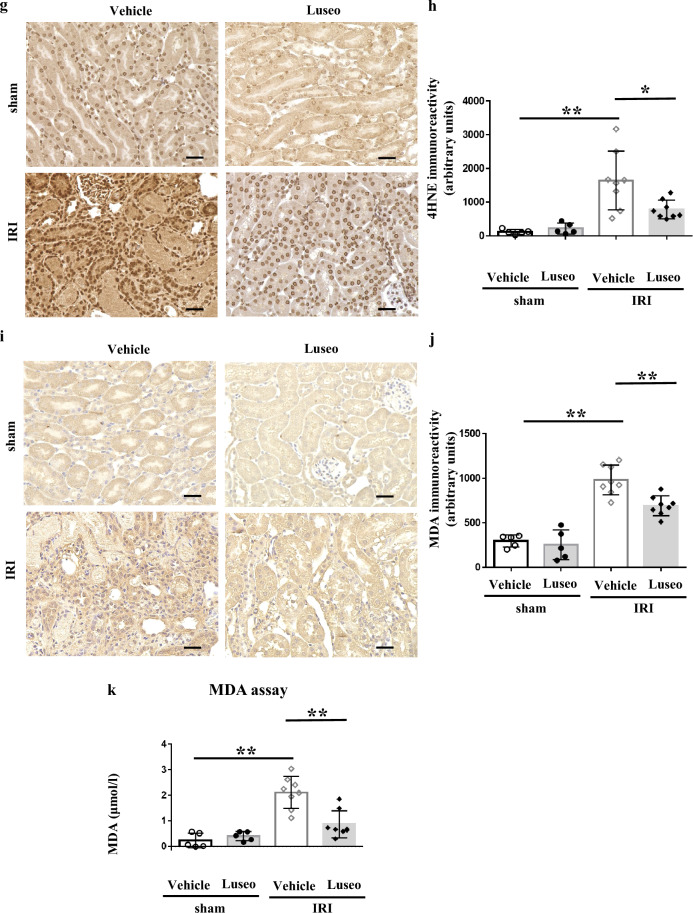
Sodium-glucose cotransporter 2 (SGLT2) inhibitors have been shown to be renoprotective in ischemia-reperfusion (I/R) injury, with several proposed mechanisms, though additional mechanisms likely exist. This study investigated the impact of luseogliflozin on kidney fibrosis at 48 h and 1 week post I/R injury in C57BL/6 mice. Luseogliflozin attenuated kidney dysfunction and the acute tubular necrosis score on day 2 post I/R injury, and subsequent fibrosis at 1 week, as determined by Sirius red staining. Metabolomics enrichment analysis of I/R-injured kidneys revealed suppression of the glycolytic system and activation of mitochondrial function under treatment with luseogliflozin. Western blotting showed increased nutrient deprivation signaling with elevated phosphorylated AMP-activated protein kinase and Sirtuin-3 in luseogliflozin-treated kidneys. Luseogliflozin-treated kidneys displayed increased protein levels of carnitine palmitoyl transferase 1α and decreased triglyceride deposition, as determined by oil red O staining, suggesting activated fatty acid oxidation. Luseogliflozin prevented the I/R injury-induced reduction in nuclear factor erythroid 2-related factor 2 activity. Western blotting revealed increased glutathione peroxidase 4 and decreased transferrin receptor protein 1 expression. Immunostaining showed reduced 4-hydroxynonenal and malondialdehyde levels, especially in renal tubules, indicating suppressed ferroptosis. Luseogliflozin may protect the kidney from I/R injury by inhibiting ferroptosis through oxidative stress reduction.
Keywords: Ferroptosis; Ischemia reperfusion injury; Luseogliflozin; Nrf2.
© 2024. The Author(s).
Conflict of interest statement
This work received the research grant by Taisho Pharmaceutical Co., the manufacturer of luseogliflozin. The funding entity did not participate in the study's design, data gathering and analysis, decision to publish, or manuscript preparation, with the sole exception of supplying pharmacokinetic data for luseogliflozin. All the authors declare no conflict of interest.
Figures





References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
