

Duropathy as a rare motor neuron disease mimic: from bibrachial amyotrophy to infratentorial superficial siderosis
- PMID: 39223525
- PMCID: PMC11367770
- DOI: 10.1186/s12883-024-03799-6
Duropathy as a rare motor neuron disease mimic: from bibrachial amyotrophy to infratentorial superficial siderosis
Abstract
Background: Bibrachial amyotrophy associated with an extradural CSF collection and infratentorial superficial siderosis (SS) are rare conditions that may occasionally mimic ALS. Both disorders are assumed to be due to dural tears.
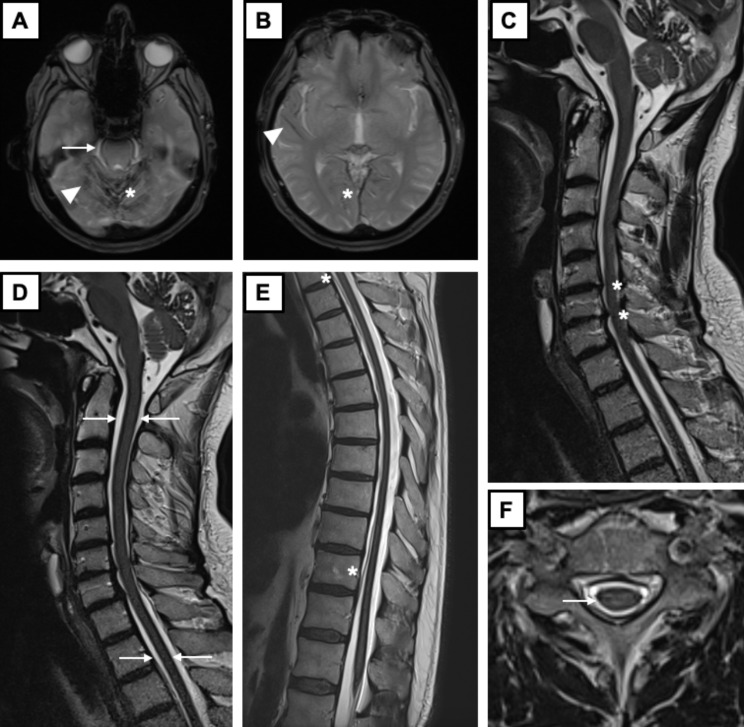
Case presentation: A 53-year-old man presented with a 7-year history of slowly progressive asymmetric bibrachial amyotrophy. Initially, a diagnosis of atypical motor neuron disease (MND) was made. At re-evaluation 11 years later, upper limb wasting and weakness had further progressed and were accompanied by sensorineural hearing loss. MRI of the brain and spine demonstrated extensive supra- and infratentorial SS (including the surface of the whole spinal cord) as well as a ventral longitudinal intraspinal fluid collection (VLISFC) extending along almost the entire thoracic spine. Osteodegenerative changes were observed at C5-C7 level, with osteophytes protruding posteriorly. The bony spurs at C6-C7 level were hypothesized to have lesioned the dura, causing a CSF leak and thus a VLISFC. Review of the MRI acquired at first evaluation showed that the VLISFC was already present at that time (actually beginning at C7 level), whereas the SS was not. 19 years after the onset of upper limb weakness, the patient additionally developed parkinsonism. Response to levodopa, brain scintigraphy with 123I-ioflupane and brain MRI with nigrosome 1 evaluation were consistent with idiopathic Parkinson's disease (PD). On the latest follow-up 21 years after symptom onset, the VLISFC was unchanged, as were upper arm weakness and wasting.
Conclusions: Based on the long-term follow-up, we could establish that, while the evidence of the VLISFC was concomitant with the clinical presentation of upper limb amyotrophy and weakness, the radiological signs of SS appeared later. This suggests that SS was not per se the cause of the ALS-like clinical picture, but rather a long-term sequela of a dural leak. The latter was instead the causative lesion, giving rise to a VLISFC which compressed the cervical motor roots. Dural tears can actually cause several symptoms, and further studies are needed to elucidate the pathophysiological correlates of "duropathies". Finally, as iron metabolism has been implicated in PD, the co-occurrence of PD with SS deserves further investigation.
Keywords: ALS mimics; Bibrachial amyotrophy; Dural leak; Duropathy; Superficial siderosis; Ventral longitudinal intraspinal fluid collection.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Hamill RC. Report of a case of melanosis of the brain, cord and meninges. J Nerv Ment Dis 1908; 35(9).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
