

Comparing the outcomes of in-vitro fertilization in patients receiving vaginal, subcutaneous, and intramuscular progesterone for luteal phase support: a three-armed randomized controlled trial
- PMID: 39223536
- PMCID: PMC11367876
- DOI: 10.1186/s12905-024-03337-z
Comparing the outcomes of in-vitro fertilization in patients receiving vaginal, subcutaneous, and intramuscular progesterone for luteal phase support: a three-armed randomized controlled trial
Abstract
Background: The optimal approach to luteal-phase support in infertility treatment remains a subject of debate. This study was conducted to investigate the clinical outcomes, side effects, and patient satisfaction associated with vaginal, subcutaneous, and intramuscular progesterone administration in infertile women undergoing Frozen Embryo Transfer (FET).
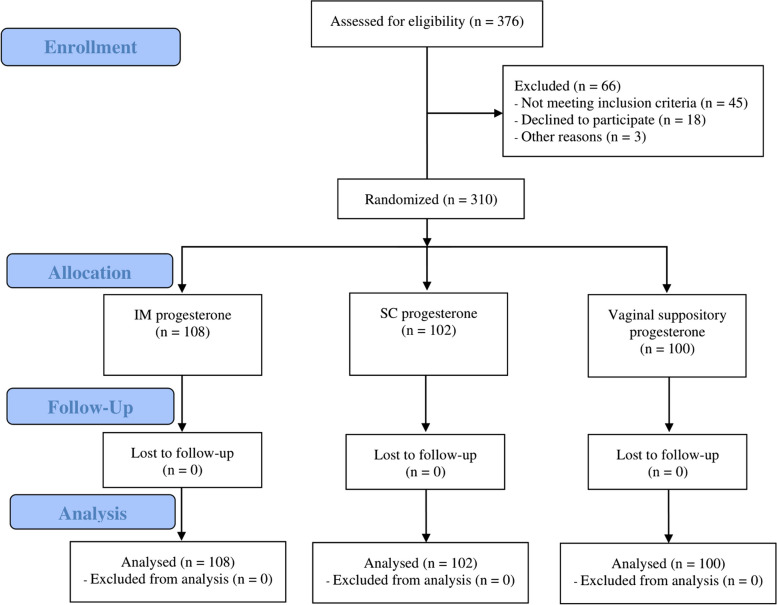
Methods: This three-armed randomized clinical trial assigned infertile patients eligible for FET to three progesterone treatment groups: vaginal suppositories (400 mg twice daily; n = 100), subcutaneous injections (25 mg daily; n = 102), and intramuscular injections (50 mg daily; n = 108). The primary outcomes were chemical and clinical pregnancy rates per embryo transfer cycle, with chemical pregnancy defined as beta-human chorionic gonadotropin levels > 50 IU/mL two weeks post-transfer and clinical pregnancy confirmed by ultrasound four weeks later. Exploratory outcomes included progesterone-related adverse effects and participant satisfaction, assessed via a Likert-scale survey 12 weeks post-transfer. Statistical analyses included Chi-square tests for categorical data, one-way analysis of variances, and Kruskal-Wallis tests for continuous data.
Results: The intramuscular progesterone group had significantly higher chemical pregnancy rates compared to the vaginal and subcutaneous groups (41.7% vs. 26.0% and 27.5%, respectively; p = 0.026). Although the clinical pregnancy rate was also higher in the intramuscular group (32.4%) compared to the vaginal (23.0%) and subcutaneous groups (21.6%), this difference was not statistically significant (p = 0.148). Additionally, patient satisfaction was greater with vaginal and subcutaneous applications than with intramuscular injections (p < 0.001), likely due to a significantly higher incidence of side effects, such as pain and edema at the injection site, in the intramuscular group (p < 0.001).
Conclusions: We found that intramuscular progesterone resulted in higher chemical pregnancy rates than vaginal or subcutaneous routes, but this did not translate into higher clinical pregnancy rates. Despite its effectiveness, intramuscular administration was associated with more adverse effects and lower patient satisfaction. Future research should explore optimizing progesterone regimens to balance efficacy and patient comfort.
Trial registration: The trial protocol was registered on December 6, 2020, in the Iranian Registry of Clinical Trials (IRCT), a primary registry in the World Health Organization (WHO) Registry Network, under the registration number IRCT20141217020351N12.
Keywords: Embryo Transfer; In Vitro Fertilization; Infertility; Luteal-phase Support; Progesterone.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- López Regalado ML, Clavero A, Gonzalvo MC, Serrano M, Martínez L, Mozas J, et al. Cumulative live birth rate after two single frozen embryo transfers (eSFET) versus a double frozen embryo transfer (DFET) with cleavage stage embryos: a retrospective cohort study. J Assist Reprod Genet. 2014;31(12):1621–7. 10.1007/s10815-014-0346-5 - DOI - PMC - PubMed
-
- Pouget O, Scalici E, Hoa-Ferrieres A, Deutsch-Bringer S, Gala A, Dechaud H, et al. Comparison of frozen embryo transfer outcomes at blastocyst stage according to freezing method and type of endometrial preparation. Gynecol Obstet Fertil. 2015;43(3):219–24. 10.1016/j.gyobfe.2015.01.012 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
