

Forme fruste keratoconus detection with OCT corneal topography using artificial intelligence algorithms
- PMID: 39223730
- PMCID: PMC11556849
- DOI: 10.1097/j.jcrs.0000000000001542
Forme fruste keratoconus detection with OCT corneal topography using artificial intelligence algorithms
Abstract
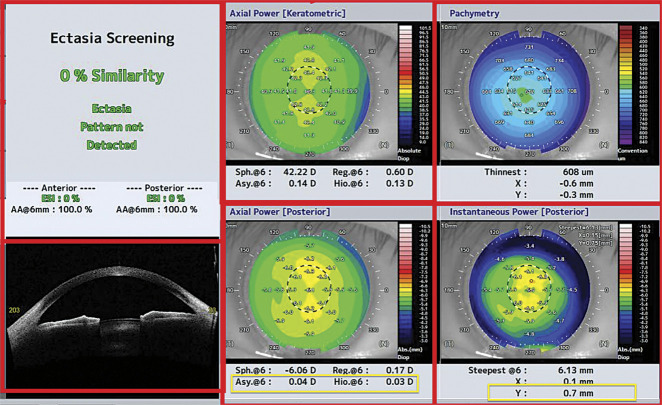
Purpose: To differentiate a normal cornea from a forme fruste keratoconus (FFKC) with the swept-source optical coherence tomography (SS-OCT) topography CASIA 2 using machine learning artificial intelligence algorithms.
Setting: Monocentric, performed in CHU Bordeaux, Bordeaux, France.
Design: Retrospective case-control.
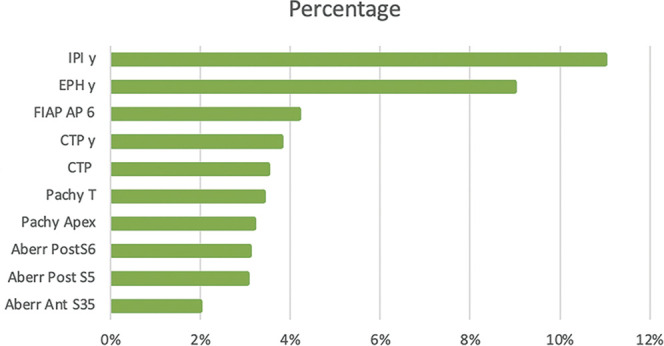
Methods: 3 groups were included: KC group (108 eyes), FFKC (88 eyes), and normal corneas (162 eyes). The data were analyzed and processed using the Dataiku data science platform. Machine learning models (random forest [RF], logistic regression [LR]) were used to develop a multiclass classifier for automated early KC detection. The models were trained using a training database and tested using a test database. Then, algorithms were compared with the Ectasia Screening Index (ESI), which is an OCT-topography inherent screening score for ectasia.
Results: The LR and RF detected FFKC with an area under the curve of 0.99 and 0.98, respectively. The sensitivities of LR (100%) and RF (84%) were better than the ESI (28%) for the diagnosis of FFKC. However, ESI has a maximum specificity (100%) compared with the LR (100%) and 90% for RF.
Conclusions: This study identified discriminating topographic parameters to be considered in refractive surgery screening on SS-OCT CASIA 2. An algorithm capable of classifying normal eyes vs FFKC cases was developed, with improved performance compared with the ESI score.
Copyright © 2024 Published by Wolters Kluwer on behalf of ASCRS and ESCRS.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
