

Coronary coding in dTGA pre- and post-ASO-verification and necessary corrections following adult CMR
- PMID: 39224101
- PMCID: PMC11367965
- DOI: 10.1093/ehjimp/qyae055
Coronary coding in dTGA pre- and post-ASO-verification and necessary corrections following adult CMR
Abstract
Aims: In adult patients with transposition of the great arteries (dTGA) after arterial switch operation (ASO), the coronary artery circulation after neonatal surgical transfer remains a major culprit for long-term sequelae, including myocardial ischaemia and sudden cardiac death. As coronary imaging in paediatric age is often incomplete and classification mainly relies on the surgeon's description in the operation report, we intended to develop a systematic, understandable pattern of the coronary status for each young patient, combining unambiguous coding with non-invasive imaging.
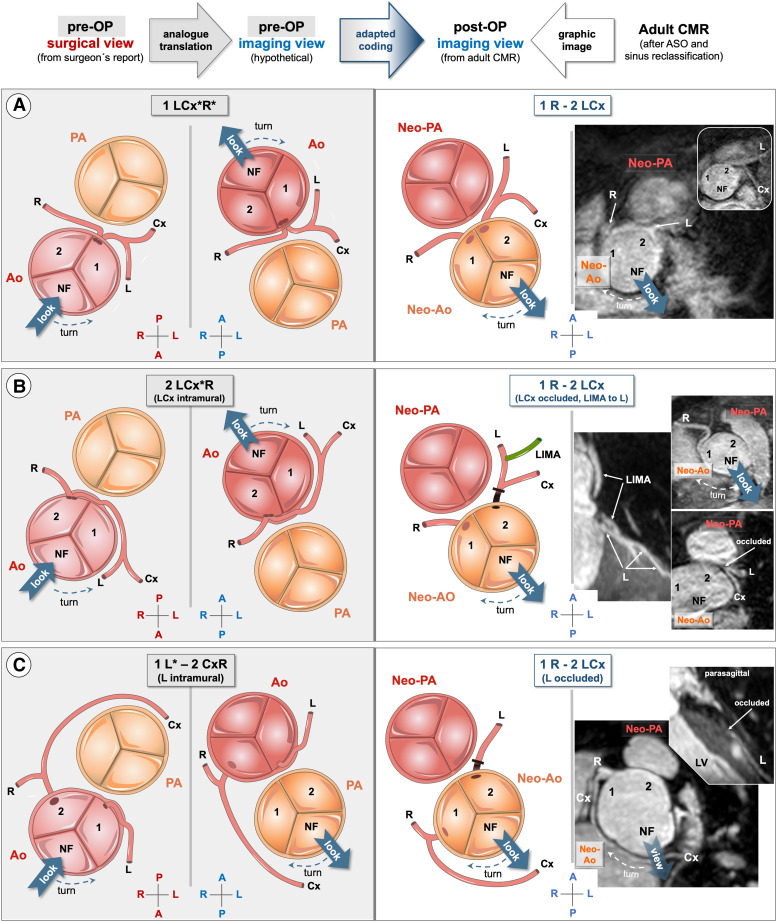
Methods and results: The monocentric prospective study evaluated 89 young adults (mean 23 years) after ASO for dTGA including cardiac magnetic resonance (CMR) coronary angiography. Following 'The Leiden Convention coronary coding system', we describe the systematic transformation process and provide a graphical illustration considering surgical and imaging views for the six main coronary types, followed by a comparison with adult CMR. Discordance between surgeon's and CMR classification is evaluated.In seven (7.9%) patients, a discordance between the surgeon's post-operative and the CMR classification was found; therefore, the initial classification had to be corrected according to adult CMR. Three cases (3.4%) with particularly challenging coronary variants (intramural and interarterial course, functional common ostium) are presented.
Conclusion: Considering the risks of a possible neonatal coronary misclassification and of increasing additional acquired coronary artery disease with age, reliable cooperation between surgeons, cardiologists, and imaging specialists must be ensured. Therefore, after completion of growth, a systematic pattern of the coronary artery status, combining unambiguous coding with CMR imaging, should be established for each patient.
Keywords: Leiden convention coronary coding system; arterial switch operation; cardiac magnetic resonance tomography; coronary artery classification; dextro-transposition of the great arteries.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interests: Any conflicts of interest have been disclosed for all authors
Figures



References
-
- Fricke TA, Buratto E, Weintraub RG, Bullock A, Wheaton G, Grigg Let al. . Long-term outcomes of the arterial switch operation. J Thorac Cardiovasc Surg 2022;163:212–9. - PubMed
-
- Shaher RM, Puddu GG. Coronary arterial anatomy in complete transposition of the great vessels. Am J Cardiol 1966;1:355–61. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials