

De-intensification of postoperative radiotherapy in head and neck cancer irrespective of human papillomavirus status-results of a prospective multicenter phase II trial (DIREKHT Trial)
- PMID: 39224800
- PMCID: PMC11366634
- DOI: 10.3389/fonc.2024.1447123
De-intensification of postoperative radiotherapy in head and neck cancer irrespective of human papillomavirus status-results of a prospective multicenter phase II trial (DIREKHT Trial)
Abstract
Background: Current standard treatment concepts in head and neck squamous cell carcinoma (HNSCC) are based on former studies using 2D and 3D treatment plans. However, modern radiation techniques allow for a more precise and individual dose application. Therefore, in a clearly defined patient population, de-intensified risk-adapted radiation is investigated.
Methods: Patients with newly diagnosed HNSCC after surgery (with resection margins ≥1 mm and cM0) with the following tumor stages (TNM 7th Edition) were eligible for the study: oral cavity, oropharynx, or larynx: pT1-3, pN0-pN2b; hypopharynx: pT1-2, pN1. The patients should have either a low risk of local recurrence [≤pT2, resection margin ≥5 mm, no peritumoral lymphangiosis (L0), and no perineural invasion] or contralateral lymph node metastasis (≤3 ipsilateral lymph node metastases, in case of well-lateralized oropharyngeal or oral cavity cancer contralateral cN0, otherwise pN0). Patients were assigned to three different treatment regimes with reduction of the treated volume, radiation dose, or both, according to tumor stage and results of surgery performed. The primary objective was to show an LRR of <10% after 2 years.
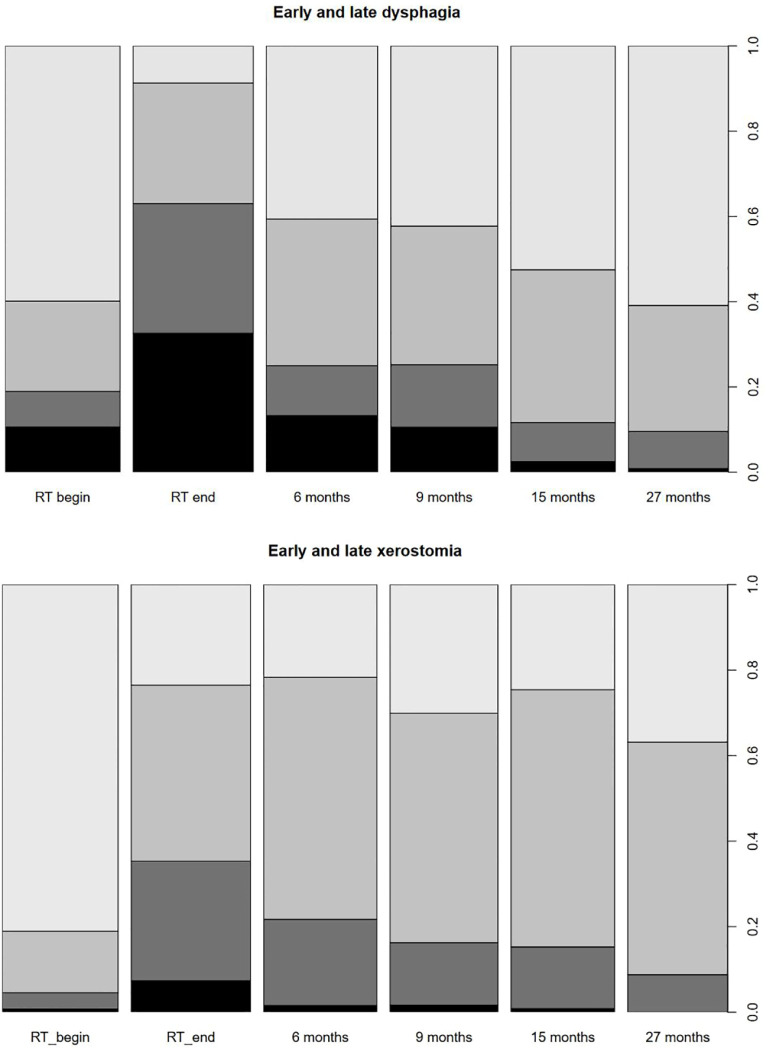
Findings: A total of 150 patients were enrolled. Tumor localizations were as follows: n = 53 (35.3%), oral cavity; n = 94 (62.7%), oropharynx (82% HPV-positive); n = 2 (1.3%), hypopharynx; and n = 1 (0.7%), larynx. A total of 61 patients (41.0%) were stage IVA, 81 (54.0%) were stage III, and 8 (5.3%) were stage II. Median follow-up was 36 months. Cumulative incidence of 2y-LRR was 5.6% (95% CI: 1.7%-9.2%) in the whole study population and 14.1% (95% CI: 3.8%-23.2%) in patients with oral cavity cancer. Cumulative incidence of 2y-LRR in non-irradiated or dose-reduced regions was 3.5% (95% CI: 0.4%-6.5%). After 2 years, disease-free survival was 92% (95% CI: 87%-96%) and overall survival was 94% (95% CI: 90%-98%) for the complete study cohort. Acute III° toxicity was as follows: dysphagia, 30%; xerostomia, 7%; mucositis, 19%; and dermatitis, 4%. Dysphagia and xerostomia decrease over time. After 27 months, late dysphagia III° and xerostomia II° were 1% and 9%, respectively.
Interpretation: The study met its primary objective. De-intensification of postoperative radiotherapy irrespective of HPV status in a predefined patient population is associated with a favorable toxicity profile without compromising LRR. In an unplanned subgroup analysis, a significantly increased risk of LRR was observed in patients with oral cavity cancer. In these patients, de-intensified radiotherapy should be applied with caution.
Keywords: HPV; de-intensification; head and neck cancer; postoperative; radiotherapy.
Copyright © 2024 Haderlein, von der Grün, Balermpas, Rödel, Hautmann, Steger, Bohr, Hehr, Stromberger, Budach, Schymalla, Engenhart-Cabillic, Kocik, Geinitz, Nestle, Klautke, Scherl, Gall, Frey, Schubert, Semrau, Ott, Kesting, Iro, Mueller and Fietkau.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures





References
-
- Bjordal K, de Graeff A, Fayers PM, Hammerlid E, van Pottelsberghe C, Curran D, et al. . A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur J Cancer. (2000) 36:1796–807. doi: 10.1016/S0959-8049(00)00186-6 - DOI - PubMed
-
- Oskam IM, Verdonck-de Leeuw IM, Aaronson NK, Witte BI, de Bree R, Doornaert P, et al. . Prospective evaluation of health-related quality of life in long-term oral and oropharyngeal cancer survivors and the perceived need for supportive care. Oral Oncol. (2013) 49:443–8. doi: 10.1016/j.oraloncology.2012.12.005 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous