

Increased risk of kidney failure in patients with genetic kidney disorders
- PMID: 39225089
- PMCID: PMC11364380
- DOI: 10.1172/JCI178573
Increased risk of kidney failure in patients with genetic kidney disorders
Abstract
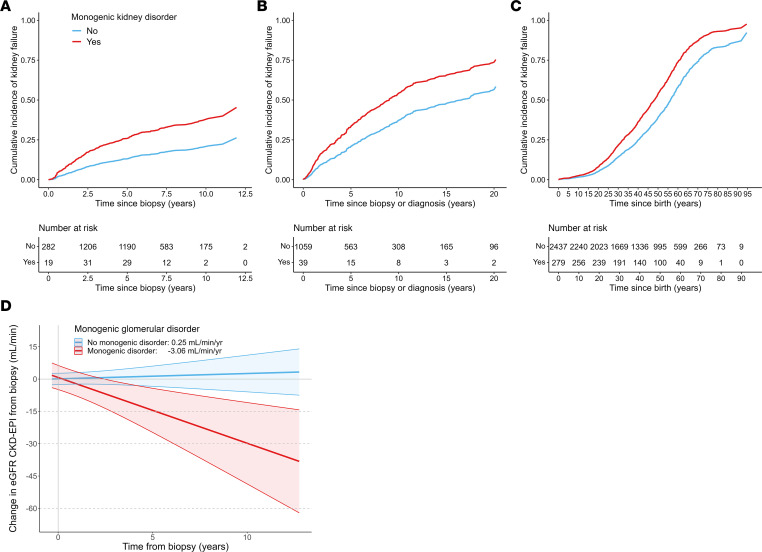
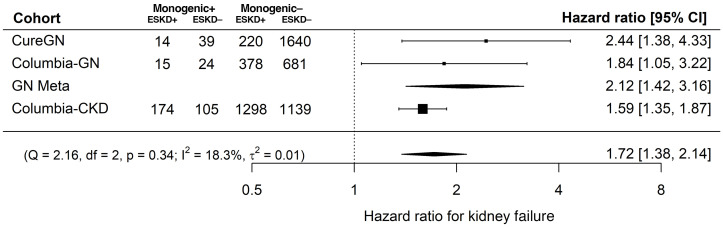
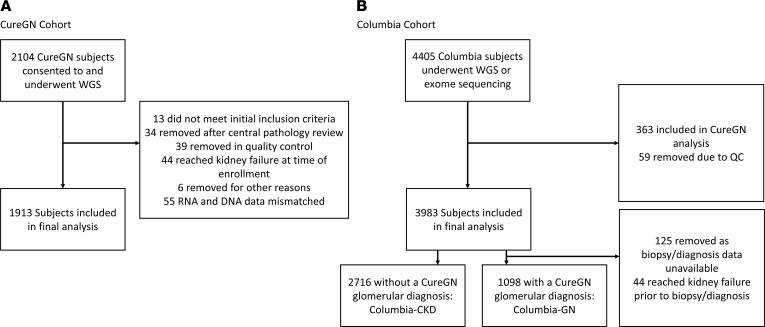
BACKGROUNDIt is unknown whether the risk of kidney disease progression and failure differs between patients with and without genetic kidney disorders.METHODSThree cohorts were evaluated: the prospective Cure Glomerulonephropathy Network (CureGN) and 2 retrospective cohorts from Columbia University, including 5,727 adults and children with kidney disease from any etiology who underwent whole-genome or exome sequencing. The effects of monogenic kidney disorders and APOL1 kidney-risk genotypes on the risk of kidney failure, estimated glomerular filtration rate (eGFR) decline, and disease remission rates were evaluated along with diagnostic yields and the impact of American College of Medical Genetics secondary findings (ACMG SFs).RESULTSMonogenic kidney disorders were identified in 371 patients (6.5%), high-risk APOL1 genotypes in 318 (5.5%), and ACMG SFs in 100 (5.2%). Family history of kidney disease was the strongest predictor of monogenic disorders. After adjustment for traditional risk factors, monogenic kidney disorders were associated with an increased risk of kidney failure (hazard ratio [HR] = 1.72), higher rate of eGFR decline (-3.06 vs. 0.25 mL/min/1.73 m2/year), and lower risk of complete remission (odds ratioNot achieving CR = 5.25). High-risk APOL1 genotypes were associated with an increased risk of kidney failure (HR = 1.67) and faster eGFR decline (-2.28 vs. 0.25 mL/min/1.73 m2), replicating prior findings. ACMG SFs were not associated with personal or family history of associated diseases, but were predicted to impact care in 70% of cases.CONCLUSIONSMonogenic kidney disorders were associated with an increased risk of kidney failure, faster eGFR decline, and lower rates of complete remission, suggesting opportunities for early identification and intervention based on molecular diagnosis.TRIAL REGISTRATIONNA.FUNDINGNational Institute of Diabetes and Digestive and Kidney Diseases grants U24DK100845 (formerly UM1DK100845), U01DK100846 (formerly UM1DK100846), U01DK100876 (formerly UM1DK100876), U01DK100866 (formerly UM1DK100866), U01DK100867 (formerly UM1DK100867), U24DK100845, DK081943, RC2DK116690, 2U01DK100876, 1R01DK136765, 5R01DK082753, and RC2-DK122397; NephCure Kidney International; Department of Defense Research Awards PR201425, W81XWH-16-1-0451, and W81XWH-22-1-0966; National Center for Advancing Translational Sciences grant UL1TR001873; National Library of Medicine grant R01LM013061; National Human Genome Research Institute grant 2U01HG008680.
Keywords: Chronic kidney disease; Genetic diseases; Genetics; Molecular diagnosis; Nephrology.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
