

The Role of Active and Passive Smoking in Chronic Obstructive Pulmonary Disease and Systemic Inflammation: A 12-year Prospective Study in China
- PMID: 39225766
- PMCID: PMC11442906
- DOI: 10.1007/s44197-024-00290-w
The Role of Active and Passive Smoking in Chronic Obstructive Pulmonary Disease and Systemic Inflammation: A 12-year Prospective Study in China
Abstract
Background: There is no consensus on the cause and effect of systemic chronic inflammation (SCI) regarding chronic obstructive pulmonary disease (COPD). The impact of second-hand smoke (SHS) on COPD has reached inconsistent conclusions.
Methods: The China Kadoorie Biobank cohort was followed up from the 2004-08 baseline survey to 31 December 2018. Among the selected 445,523 participants in the final analysis, Cox and linear regressions were performed to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) of tobacco exposure with COPD risk and baseline levels of log-transformed inflammatory factors [βs (95% CIs)], respectively.
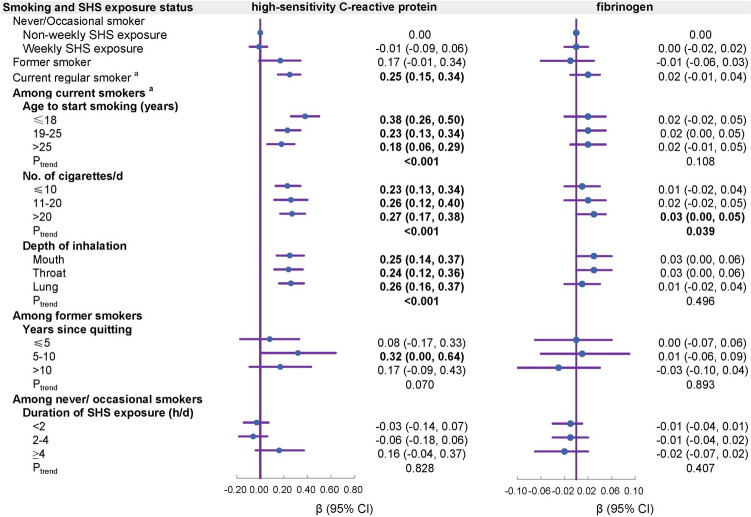
Results: Participants were followed up for a median of 12.1 years and 11,825 incident COPD events were documented. Ever-smokers were associated with a higher risk of COPD than non-smokers with non-weekly SHS exposure. A younger age to start smoking, a greater amount of daily tobacco consumption, and deeper inhalation were associated with increased risk of COPD and correlated with elevated levels of plasma high-sensitivity C-reactive protein (hs-CRP, all Ptrend < 0.001) even two years before COPD onset. Among former smokers, COPD risk declined with longer smoking cessation (Ptrend < 0.001) and those quitting smoking for over ten years presented no difference in COPD risk and hs-CRP level from non-smokers [HR (95% CI) = 1.05 (0.89, 1.25), β (95% CI) = 0.17 (- 0.09, 0.43)]. Among non-smokers, weekly SHS exposure was associated with a slightly higher COPD risk [HR (95% CI) = 1.06 (1.01, 1.12)].
Conclusions: Incremental exposure to tobacco smoke was related to elevated SCI level before COPD onset, then an increase in COPD susceptibility. Quitting smoking as early as possible is suggested as a practical approach to reducing COPD risk in smokers. Given the high prevalence of both COPD and SHS exposure, the risk associated with SHS exposure deserves attention.
Keywords: Active smoking; Chronic obstructive pulmonary disease; Passive smoking; Prospective cohort study; Systemic inflammation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Disease GIfCOL: Global strategy for the diagnosis, management, and prevention of COPD: 2023 report. In.; 2022.
-
- Ge J, Xu Y, Wang C. Internal Medicine (9th edition). Beijing: People’s Medical Publishing House; 2018.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
