

Neurological Symptoms and Cause of Death Among Young Children in Low- and Middle-Income Countries
- PMID: 39226053
- PMCID: PMC11372484
- DOI: 10.1001/jamanetworkopen.2024.31512
Neurological Symptoms and Cause of Death Among Young Children in Low- and Middle-Income Countries
Abstract
Importance: The emergence of acute neurological symptoms in children necessitates immediate intervention. Although low- and middle-income countries (LMICs) bear the highest burden of neurological diseases, there is a scarcity of diagnostic and therapeutic resources. Therefore, current understanding of the etiology of neurological emergencies in LMICs relies mainly on clinical diagnoses and verbal autopsies.
Objective: To characterize the association of premortem neurological symptoms and their management with postmortem-confirmed cause of death among children aged younger than 5 years in LMICs and to identify current gaps and improve strategies to enhance child survival.
Design, setting, and participants: This cross-sectional study was conducted between December 3, 2016, and July 22, 2022, at the 7 participating sites in the Child Health and Mortality Prevention Surveillance (CHAMPS) network (Bangladesh, Ethiopia, Kenya, Mali, Mozambique, Sierra Leone, and South Africa). Minimally invasive tissue sampling was performed at the CHAMPS sites with specimens from deceased children aged younger than 5 years. This study included deceased children who underwent a premortem neurological evaluation and had a postmortem-confirmed cause of death. Data analysis was performed between July 22, 2022, and January 15, 2023.
Main outcomes and measures: Descriptive analysis was performed using neurological evaluations from premortem clinical records and from postmortem determination of cause of death (based on histopathology, microbiological testing, clinical records, and verbal autopsies).
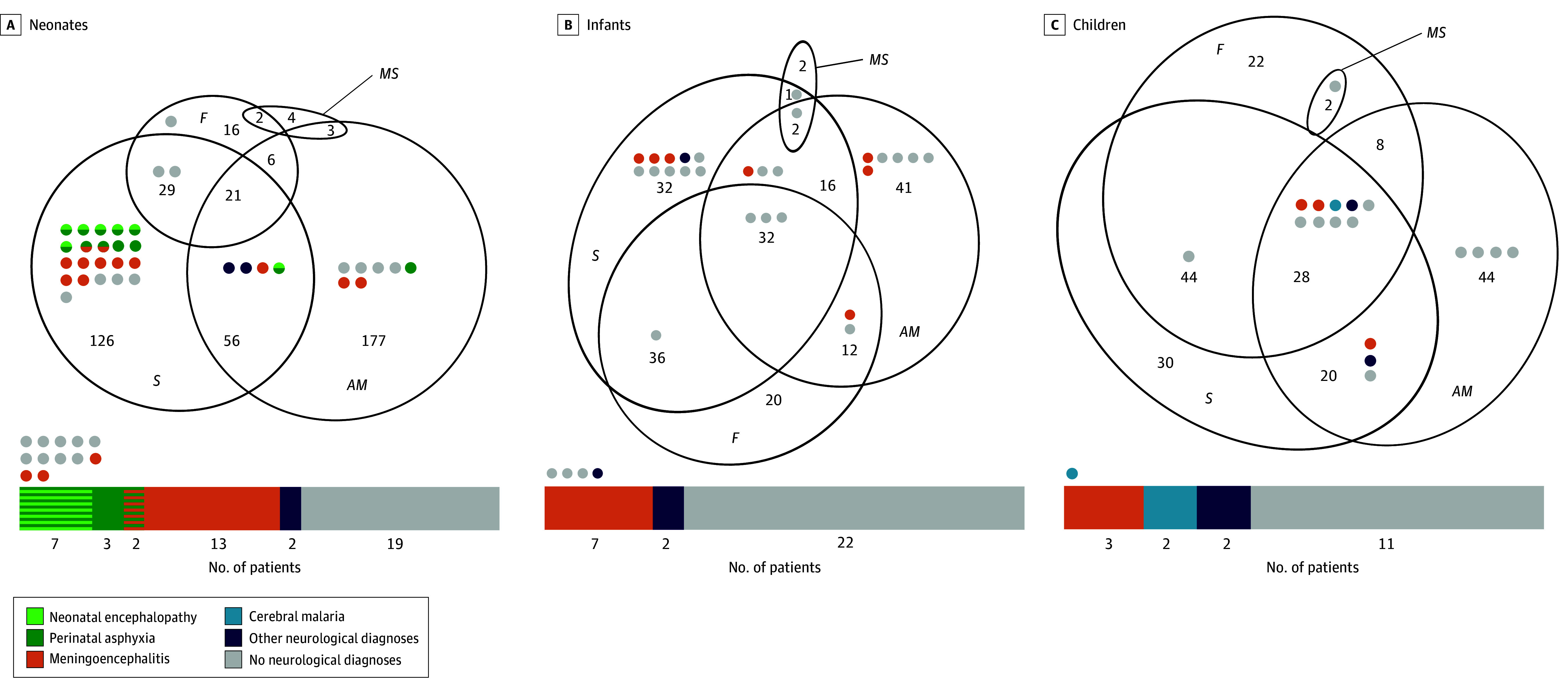
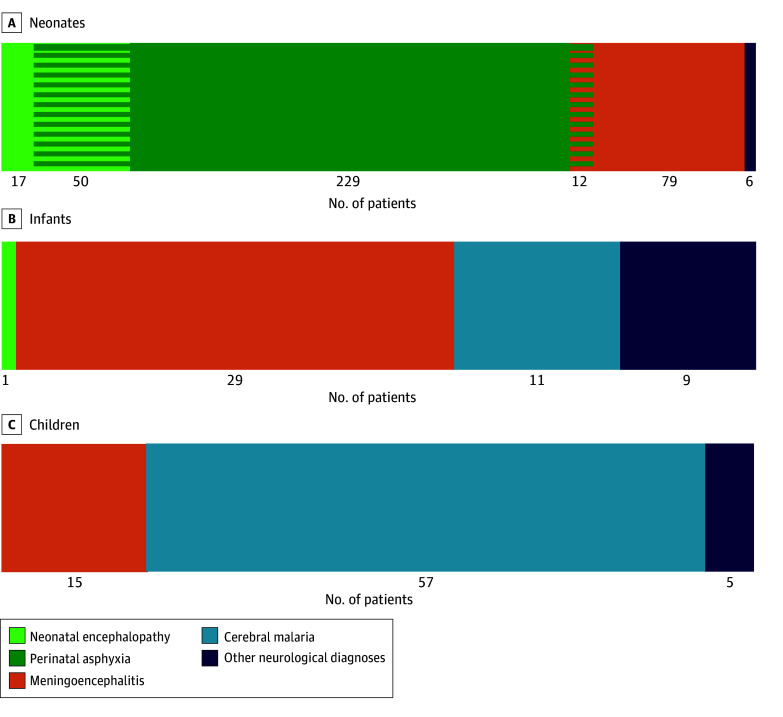
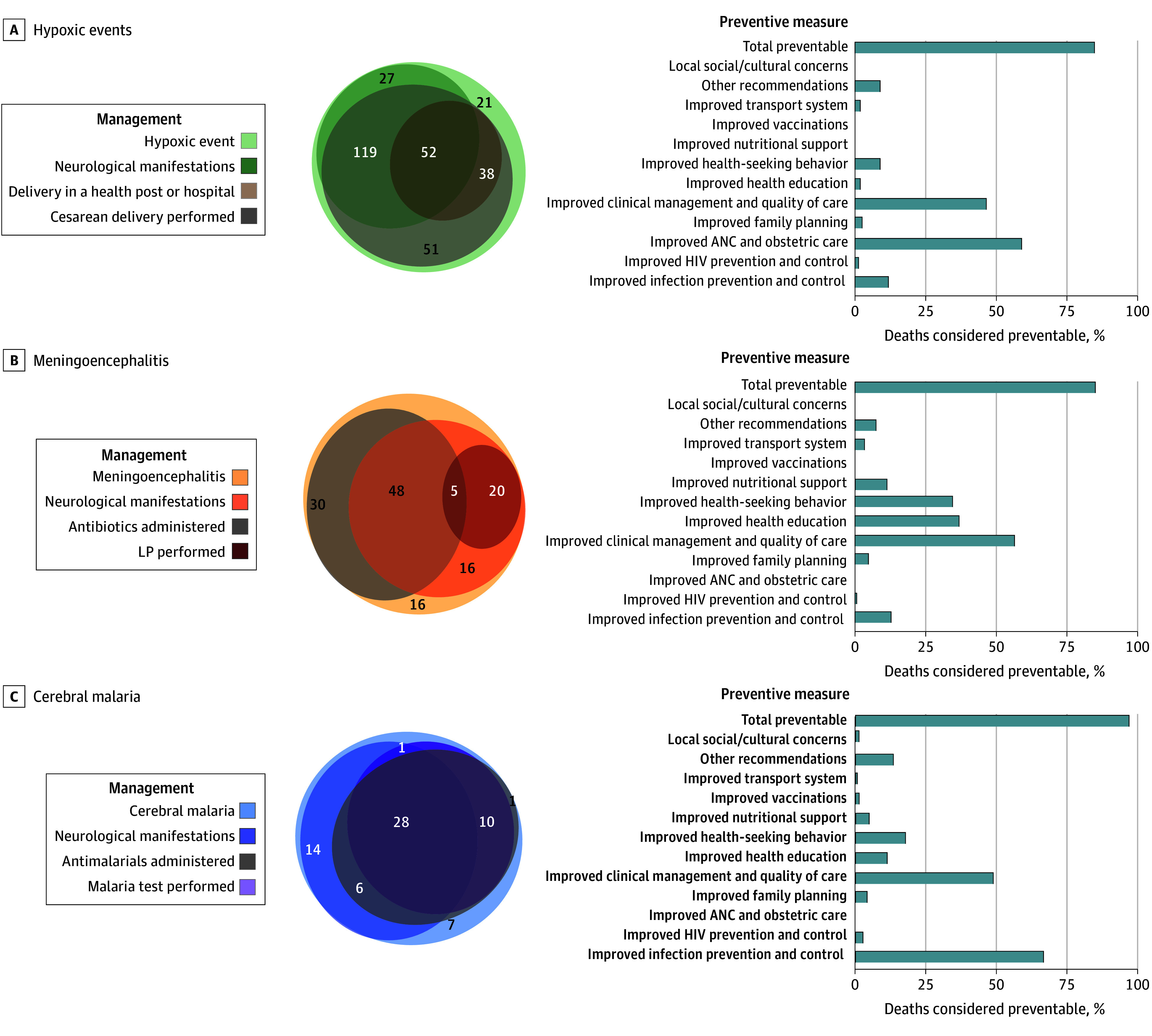
Results: Of the 2127 deaths of children codified during the study period, 1330 (62.5%) had neurological evaluations recorded and were included in this analysis. The 1330 children had a median age of 11 (IQR, 2-324) days; 745 (56.0%) were male and 727 (54.7%) presented with neurological symptoms during illness before death. The most common postmortem-confirmed neurological diagnoses related to death were hypoxic events (308 [23.2%]), meningoencephalitis (135 [10.2%]), and cerebral malaria (68 [5.1%]). There were 12 neonates with overlapping hypoxic events and meningoencephalitis, but there were no patients with overlapping meningoencephalitis and cerebral malaria. Neurological symptoms were similar among diagnoses, and no combination of symptoms was accurate in differentiating them without complementary tools. However, only 25 children (18.5%) with meningitis had a lumbar puncture performed before death. Nearly 90% of deaths (442 of 511 [86.5%]) with neurological diagnoses in the chain of events leading to death were considered preventable.
Conclusions and relevance: In this cross-sectional study of children aged younger than 5 years, neurological symptoms were frequent before death. However, clinical phenotypes were insufficient to differentiate the most common underlying neurological diagnoses. The low rate of lumbar punctures performed was especially worrying, suggesting a challenge in quality of care of children presenting with neurological symptoms. Improved diagnostic management of neurological emergencies is necessary to ultimately reduce mortality in this vulnerable population.
Conflict of interest statement
Figures
References
-
- Orman G, Rossi A, Meoded A, Huisman T. Children with acute neurological emergency. In: Hodler J, Kubik-Huch RA, von Schulthess GK, eds. Diseases of the Brain, Head and Neck, Spine 2020-2023: Diagnostic Imaging. IDKD Springer Series; 2020:179-190. doi:10.1007/978-3-030-38490-6_14 - DOI
-
- Mousa A, Al-Taiar A, Anstey NM, et al. . The impact of delayed treatment of uncomplicated P. falciparum malaria on progression to severe malaria: a systematic review and a pooled multicentre individual-patient meta-analysis. PLoS Med. 2020;17(10):e1003359. doi:10.1371/journal.pmed.1003359 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
