

Impact of structured multicentre enhanced recovery after surgery (ERAS) protocol implementation on length of stay after colorectal surgery
- PMID: 39226376
- PMCID: PMC11370790
- DOI: 10.1093/bjsopen/zrae094
Impact of structured multicentre enhanced recovery after surgery (ERAS) protocol implementation on length of stay after colorectal surgery
Abstract
Background: Increased length of stay after surgery is associated with increased healthcare utilization and adverse patient outcomes. While enhanced recovery after surgery (ERAS) protocols have been shown to reduce length of stay after colorectal surgery in trial settings, their effectiveness in real-world settings is more uncertain. The aim of this study was to assess the impact of ERAS protocol implementation on length of stay after colorectal surgery, using real-world data.
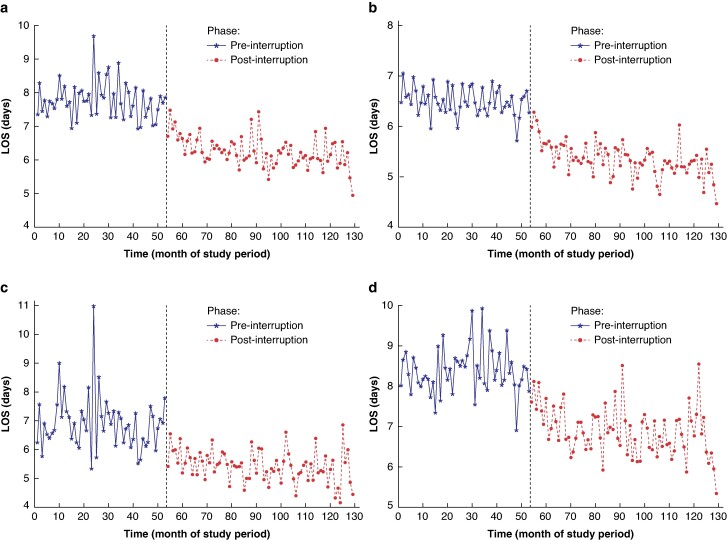
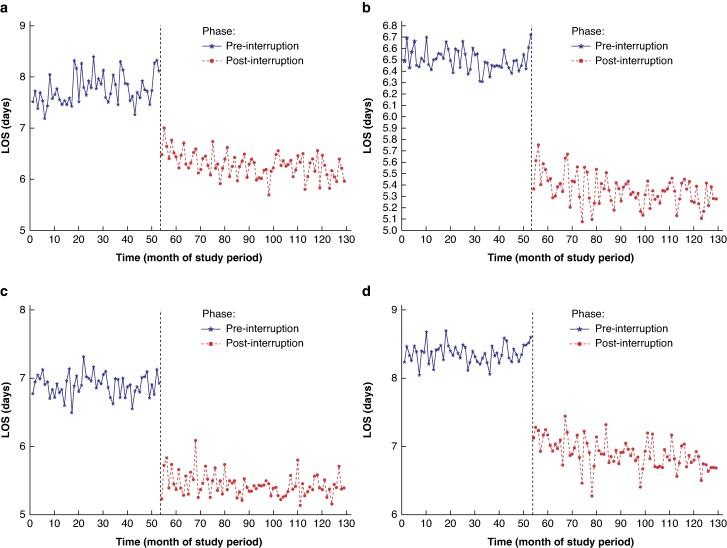
Methods: In 2012, ERAS protocols were introduced at 15 Ontario hospitals as part of the iERAS study. A cohort of patients undergoing colorectal surgery treated at these hospitals between 2008 and 2019 was created using health administrative data. Mean length of stay was computed for the intervals before and after ERAS implementation. Interrupted time series analyses were performed for predefined subgroups, namely all colorectal surgery, colorectal surgery without complications, right-sided colorectal surgery, and left-sided colorectal surgery. Sensitivity analyses were then conducted using adjusted length of stay, accounting for length of stay predictors, including: patient age, sex, marginalization, co-morbidities, and diagnosis; surgeon volume of cases, years in practice, and colorectal surgery expertise; hospital volume; and other contextual factors, including procedure type and timing, surgical approach, and in-hospital complications.
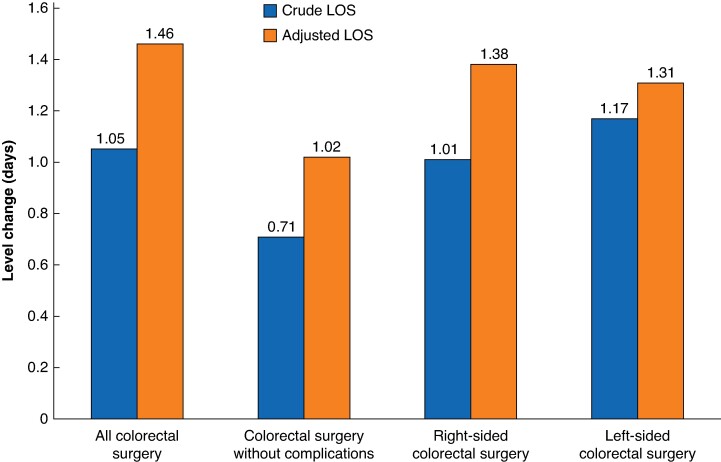
Results: A total of 32 612 patients underwent colorectal surgery during the study interval. ERAS implementation led to a decrease in length of stay of 1.05 days (13.7%). Larger decreases in length of stay were seen with more complex surgeries, with a level change of 1.17 days (15.6%) noted for the subgroup of patients undergoing left-sided colorectal surgery. The observed decreases in length of stay were durable for the length of the study interval in all analyses. When adjusting for predictors of length of stay, the effect of ERAS implementation on length of stay was larger (reduction of 1.46 days).
Conclusion: Introducing formal ERAS protocols reduces length of stay after colorectal surgery significantly, independent of temporal trends toward decreasing length of stay. These effects are durable, demonstrating that ERAS protocol implementation is an effective hospital-level intervention to reduce length of stay after colorectal surgery.
© The Author(s) 2024. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Figures
References
-
- DeWane MP, Davis KA, Schuster KM, Maung AA, Becher RD. Venous thromboembolism-related readmission in emergency general surgery patients: a role for prophylaxis on discharge? J Am Coll Surg 2018;226:1072–1077.e3 - PubMed
-
- Iannuzzi JC, Young KC, Kim MJ, Gillespie DL, Monson JRT, Fleming FJ. Prediction of postdischarge venous thromboembolism using a risk assessment model. J Vasc Surg 2013;58:1014–1020.e1 - PubMed
-
- Nielsen AW, Helm MC, Kindel T, Higgins R, Lak K, Helmen ZM et al. Perioperative bleeding and blood transfusion are major risk factors for venous thromboembolism following bariatric surgery. Surg Endosc 2018;32:2488–2495 - PubMed
-
- Suesada MM, Martins MA, Carvalho CRF. Effect of short-term hospitalization on functional capacity in patients not restricted to bed. Am J Phys Med Rehabil 2007;86:455–462 - PubMed
-
- Andrews LB, Stocking C, Krizek T, Gottlieb L, Krizek C, Vargish T et al. An alternative strategy for studying adverse events in medical care. Lancet 1997;349:309–313 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
