

Liver-related aspects of valoctocogene roxaparvovec gene therapy for hemophilia A: expert guidance for clinical practice
- PMID: 39226466
- PMCID: PMC11599981
- DOI: 10.1182/bloodadvances.2024013750
Liver-related aspects of valoctocogene roxaparvovec gene therapy for hemophilia A: expert guidance for clinical practice
Abstract
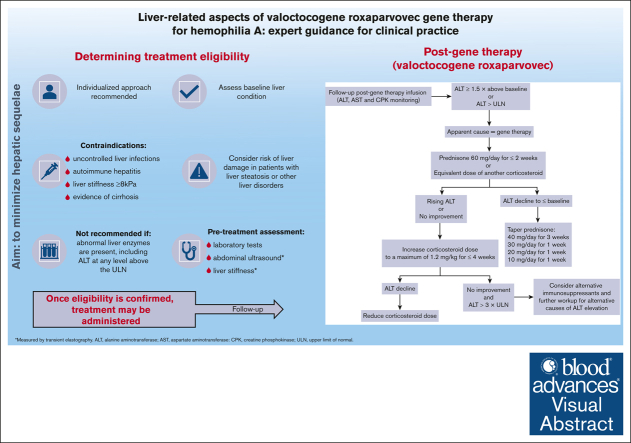
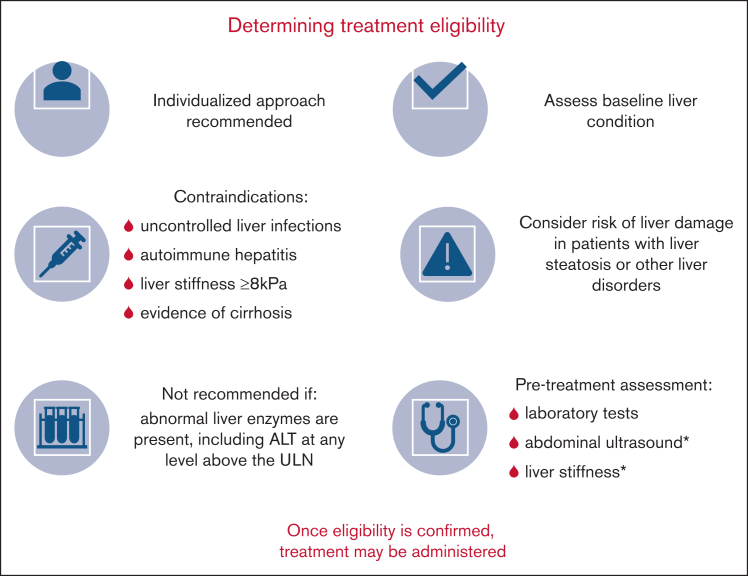
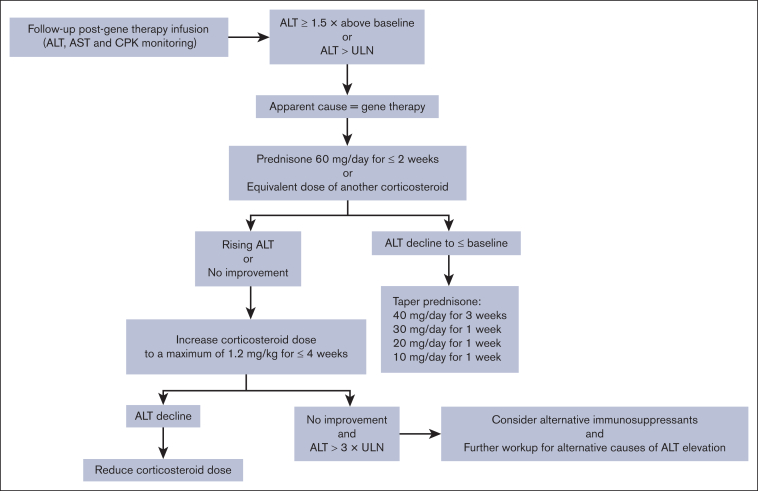
Adeno-associated virus-based gene therapy (valoctocogene roxaparvovec) is an attractive treatment for hemophilia A. Careful clinical management is required to minimize the risk of hepatotoxicity, including assessment of baseline liver condition to determine treatment eligibility and monitoring liver function after gene therapy. This article describes recommendations (developed by a group of hemophilia experts) on hepatic function monitoring before and after gene therapy. To prevent harmful liver-related effects, gene therapy is contraindicated in patients with uncontrolled liver infections, autoimmune hepatitis, liver stiffness ≥8 kPa, or cirrhosis. Before using gene therapy in patients with liver steatosis or other liver disorders, the risk of liver damage should be considered using a highly individualized approach. Treatment is not recommended in patients with abnormal liver enzymes, including alanine aminotransferase (ALT) at any level above the upper limit of normal (ULN). Therefore, pretreatment assessment of liver health should include laboratory tests, abdominal ultrasound, and liver stiffness measurements by transient elastography (TE). In the first year after therapy, ALT levels should be monitored 1 to 2 times per week to detect elevations ≥1.5× ULN, which may require immunosuppressant therapy. Patients with ALT elevation should receive prednisone 60 mg/d for 2 weeks, followed by stepwise tapering when ALT returns to baseline. ALT monitoring should continue long term (every 3-6 months), along with abdominal ultrasound (every 6 months) and TE (yearly) evaluations. When patients with good liver health are selected for treatment and closely monitored thereafter, ALT elevations can be promptly treated and are expected to resolve without long-term hepatic sequelae.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: V.L.M. is a member of advisory boards of BioMarin, CSL Behring, and Pfizer; a speaker for Gore and Alfasigma; and has received a travel grant from Sanofi and Takeda. V.C. has received a research grant from Ipsen; honoraria from Albireo Pharma, Incyte, and Revalma for seminars; and honoraria from Ipsen for participation in an advisory board meeting. G.D.M. is a member of speaker bureaus for BioMarin, Bayer, CSL Behring, Roche, Takeda, and Viatris Pharmaceuticals; and is an ad-hoc speaker/consultant for BioMarin, Bayer, Pfizer, Takeda, and Viatris Pharmaceuticals. F. Morisco is a member of advisory board for BioMarin. F.P. is a member of advisory boards for Sobi, Sanofi, Roche, CSL Behring, and BioMarin; and a speaker at education symposia organized by Takeda and Spark. C.S. is an advisory board member for BioMarin. E.Z. received fees as an advisory board member from Bayer, BioMarin, CSL Behring, Novo Nordisk, Sobi, and Takeda. G.C. is a member of advisory boards for Bayer, BioMarin, CSL Behring, LFB, Novo Nordisk, Pfizer, Roche, Sobi, and Takeda; and has been a speaker at education symposia organized by BioMarin, BIOVIIIx, CSL Behring, LFB, Roche, and Takeda. F. Marra has received travel grants from Alfasigma; consultant fees from AstraZeneca; speaker honoraria, consultant fees, and travel grants from Bayer; consultant fees from BioMarin; speaker honoraria and consultant fees from Gilead; consultant fees from Ipsen; speaker honoraria from Intercept; consultant fees from Merck Sharp & Dohme, Eisai, Menarini, Novartis, Novo Nordisk, and Roche. The remaining authors declare no competing financial interests.
Figures
References
-
- Berntorp E, Fischer K, Hart DP, et al. Haemophilia. Nat Rev Dis Primers. 2021;7(1):45. - PubMed
-
- Miesbach W, Foster GR, Peyvandi F. Liver-related aspects of gene therapy for haemophilia: call to action for collaboration between haematologists and hepatologists. J Hepatol. 2023;78(3):467–470. - PubMed
-
- Pipe SW, Shima M, Lehle M, et al. Efficacy, safety, and pharmacokinetics of emicizumab prophylaxis given every 4 weeks in people with haemophilia A (HAVEN 4): a multicentre, open-label, non-randomised phase 3 study. Lancet Haematol. 2019;6(6):e295–e305. - PubMed
