Customized Visual Discrimination Digital Therapy According to Visual Field Defects in Chronic Stroke Patients
- PMID: 39227334
- PMCID: PMC11372206
- DOI: 10.3988/jcn.2024.0015
Customized Visual Discrimination Digital Therapy According to Visual Field Defects in Chronic Stroke Patients
Abstract
Background and purpose: Visual perceptual learning (VPL) may improve visual field defects (VFDs) after chronic stroke, but the optimal training duration and location remain unknown. This prospective study aimed to determine the efficacy of 8 weeks of VFD-customized visual discrimination training in improving poststroke VFDs.
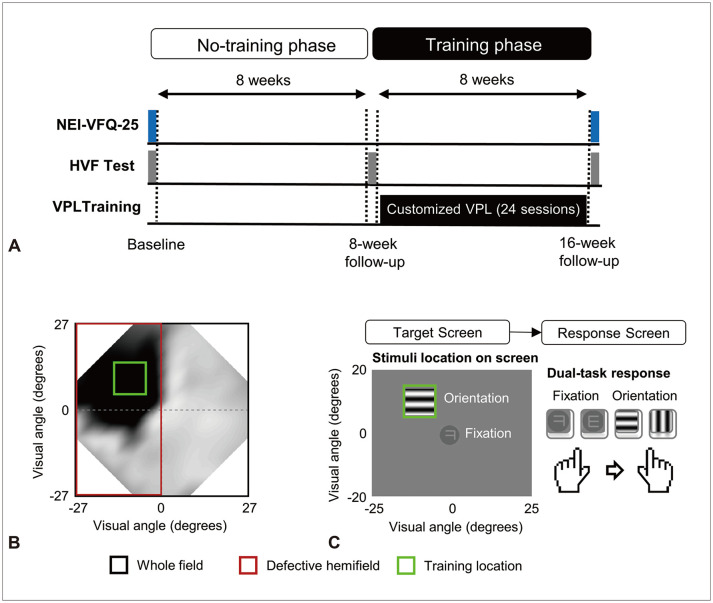
Methods: Prospectively enrolled patients with poststroke VFDs initially received no training for 8 weeks (no-training phase). They subsequently underwent our customized VPL program that included orientation-discrimination tasks in individualized blind fields and central letter-discrimination tasks three times per week for 8 weeks (training phase). We analyzed the luminance detection sensitivity and deviation as measured using Humphrey visual field tests before and after the no-training and training phases. The vision-related quality of life was assessed at baseline and at a 16-week follow-up using the National Eye Institute Visual Function Questionnaire-25 (NEI-VFQ-25).
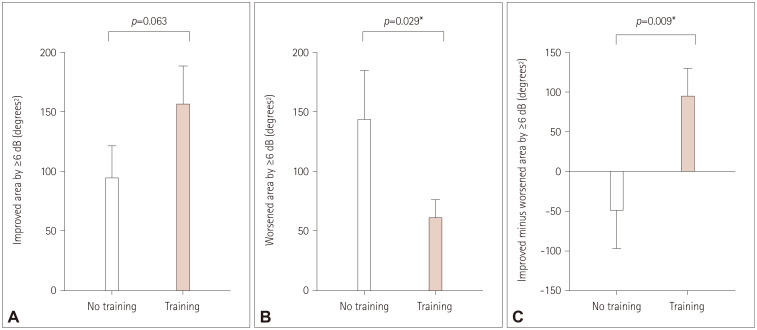
Results: Changes in mean total deviation (MTD) scores were greater during the training phase than during the no-training phase (defective hemifield, p=0.002; whole field, p=0.004). The MTD scores improved during the training phase (defective hemifield, p=0.004; whole field, p=0.016), but not during the no-training phase (defective hemifield, p=0.178; whole field, p=0.178). The difference between the improved and worsened areas (≥6 dB changes in luminance detection sensitivity) was greater during the training phase than during the no-training phase (p=0.009). The vision-specific social functioning subscore of the NEI-VFQ-25 improved after the 16-week study period (p=0.040).
Conclusions: Our 8-week VFD-customized visual discrimination training protocol may effectively improve VFDs and vision-specific social functioning in chronic stroke patients.
Keywords: cortical blindness; stroke; vision disorders; visual perception.
Copyright © 2024 Korean Neurological Association.
Conflict of interest statement
Eun-Jae Lee, a contributing editor of the
Figures


References
-
- Pollock A, Hazelton C, Henderson CA, Angilley J, Dhillon B, Langhorne P, et al. Interventions for visual field defects in patients with stroke. Cochrane Database Syst Rev. 2019;5:CD008388. - PubMed
-
- Sand KM, Wilhelmsen G, Naess H, Midelfart A, Thomassen L, Hoff JM. Vision problems in ischaemic stroke patients: effects on life quality and disability. Eur J Neurol. 2016;23(Suppl 1):1–7. - PubMed
-
- Papageorgiou E, Hardiess G, Schaeffel F, Wiethoelter H, Karnath HO, Mallot H, et al. Assessment of vision-related quality of life in patients with homonymous visual field defects. Graefes Arch Clin Exp Ophthalmol. 2007;245:1749–1758. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous