

Recombinant thrombomodulin and recombinant antithrombin attenuate pulmonary endothelial glycocalyx degradation and neutrophil extracellular trap formation in ventilator-induced lung injury in the context of endotoxemia
- PMID: 39227918
- PMCID: PMC11373098
- DOI: 10.1186/s12931-024-02958-0
Recombinant thrombomodulin and recombinant antithrombin attenuate pulmonary endothelial glycocalyx degradation and neutrophil extracellular trap formation in ventilator-induced lung injury in the context of endotoxemia
Abstract
Background: Vascular endothelial damage is involved in the development and exacerbation of ventilator-induced lung injury (VILI). Pulmonary endothelial glycocalyx and neutrophil extracellular traps (NETs) are endothelial protective and damaging factors, respectively; however, their dynamics in VILI and the effects of recombinant thrombomodulin and antithrombin on these dynamics remain unclear. We hypothesized that glycocalyx degradation and NETs are induced by VILI and suppressed by recombinant thrombomodulin, recombinant antithrombin, or their combination.
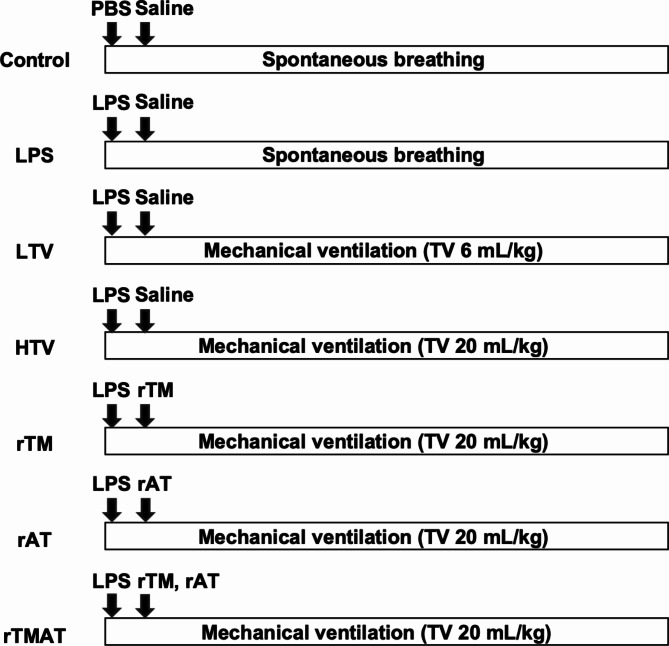
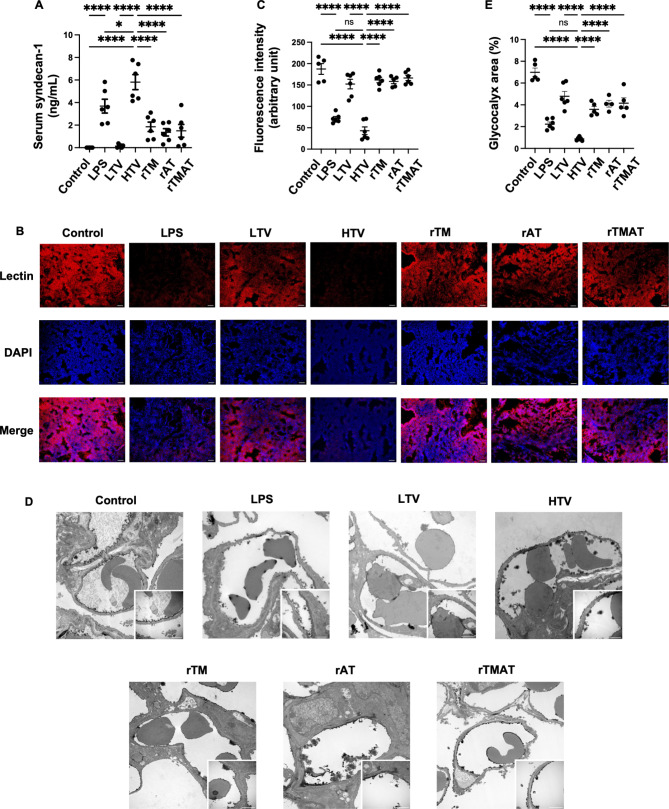
Methods: VILI was induced in male C57BL/6J mice by intraperitoneal lipopolysaccharide injection (20 mg/kg) and high tidal volume ventilation (20 mL/kg). In the intervention groups, recombinant thrombomodulin, recombinant antithrombin, or their combination was administered at the start of mechanical ventilation. Glycocalyx degradation was quantified by measuring serum syndecan-1, fluorescence-labeled lectin intensity, and glycocalyx-occupied area in the pulmonary vascular lumen. Double-stranded DNA in the bronchoalveolar fluid and fluorescent areas of citrullinated histone H3 and myeloperoxidase were quantified as NET formation.
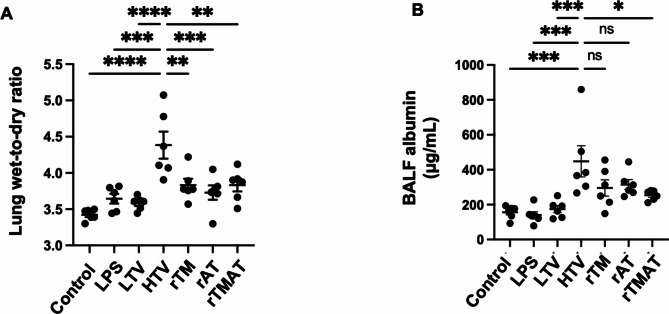
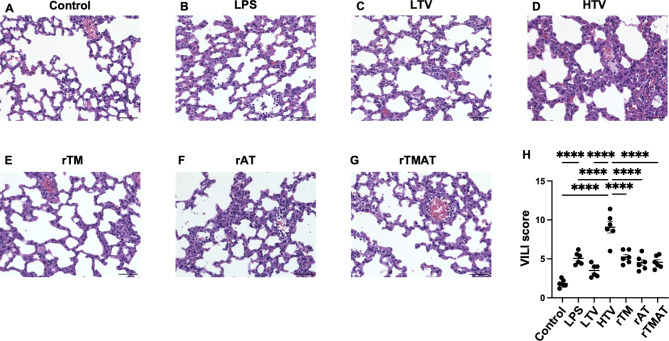
Results: Serum syndecan-1 increased, and lectin fluorescence intensity decreased in VILI. Electron microscopy revealed decreases in glycocalyx-occupied areas within pulmonary microvessels in VILI. Double-stranded DNA levels in the bronchoalveolar lavage fluid and the fluorescent area of citrullinated histone H3 and myeloperoxidase in lung tissues increased in VILI. Recombinant thrombomodulin, recombinant antithrombin, and their combination reduced glycocalyx injury and NET marker levels. There was little difference in glycocalyx injury and NET makers between the intervention groups.
Conclusion: VILI induced glycocalyx degradation and NET formation. Recombinant thrombomodulin and recombinant antithrombin attenuated glycocalyx degradation and NETs in our VILI model. The effect of their combination did not differ from that of either drug alone. Recombinant thrombomodulin and antithrombin have the potential to be therapeutic agents for biotrauma in VILI.
Keywords: Biotrauma; Glycocalyx; Neutrophil extracellular traps; Recombinant antithrombin; Recombinant thrombomodulin; Ventilator-induced lung injury.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Vascular endothelial glycocalyx shedding in ventilator-induced lung injury in rats.Microvasc Res. 2024 May;153:104658. doi: 10.1016/j.mvr.2024.104658. Epub 2024 Jan 22. Microvasc Res. 2024. PMID: 38266910
-
Simvastatin mitigates ventilator-induced lung injury in mice with acute respiratory distress syndrome via a mechanism partly dependent on neutrophil extracellular traps.Eur J Med Res. 2025 Apr 17;30(1):302. doi: 10.1186/s40001-025-02544-0. Eur J Med Res. 2025. PMID: 40247369 Free PMC article.
-
Recombinant Antithrombin Attenuates Acute Respiratory Distress Syndrome in Experimental Endotoxemia.Am J Pathol. 2021 Sep;191(9):1526-1536. doi: 10.1016/j.ajpath.2021.05.015. Epub 2021 Jun 8. Am J Pathol. 2021. PMID: 34116023 Free PMC article.
-
The endothelial glycocalyx and perioperative lung injury.Curr Opin Anaesthesiol. 2017 Feb;30(1):36-41. doi: 10.1097/ACO.0000000000000434. Curr Opin Anaesthesiol. 2017. PMID: 27941354 Review.
-
Molecular Mechanisms of Ventilator-Induced Lung Injury.Chin Med J (Engl). 2018 May 20;131(10):1225-1231. doi: 10.4103/0366-6999.226840. Chin Med J (Engl). 2018. PMID: 29553050 Free PMC article. Review.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
