

Metabolically "extremely unhealthy" obese and non-obese people with diabetes and the risk of cardiovascular adverse events: the Silesia Diabetes - Heart Project
- PMID: 39227929
- PMCID: PMC11373332
- DOI: 10.1186/s12933-024-02420-x
Metabolically "extremely unhealthy" obese and non-obese people with diabetes and the risk of cardiovascular adverse events: the Silesia Diabetes - Heart Project
Abstract
Background: There is a growing burden of non-obese people with diabetes mellitus (DM). However, their cardiovascular risk (CV), especially in the presence of cardiovascular-kidney-metabolic (CKM) comorbidities is poorly characterised. The aim of this study was to analyse the risk of major CV adverse events in people with DM according to the presence of obesity and comorbidities (hypertension, chronic kidney disease, and dyslipidaemia).
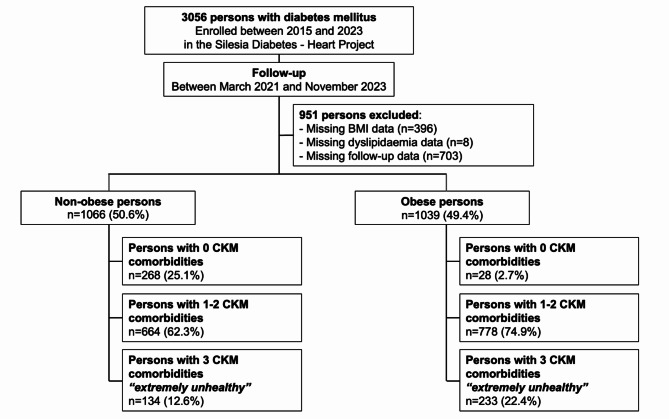
Methods: We analysed persons who were enrolled in the prospective Silesia Diabetes Heart Project (NCT05626413). Individuals were divided into 6 categories according to the presence of different clinical risk factors (obesity and CKM comorbidities): (i) Group 1: non-obese with 0 CKM comorbidities; (ii) Group 2: non-obese with 1-2 CKM comorbidities; (iii) Group 3: non-obese with 3 CKM comorbidities (non-obese "extremely unhealthy"); (iv) Group 4: obese with 0 CKM comorbidities; (v) Group 5: obese with 1-2 CKM comorbidities; and (vi) Group 6: obese with 3 CKM comorbidities (obese "extremely unhealthy"). The primary outcome was a composite of CV death, myocardial infarction (MI), new onset of heart failure (HF), and ischemic stroke.
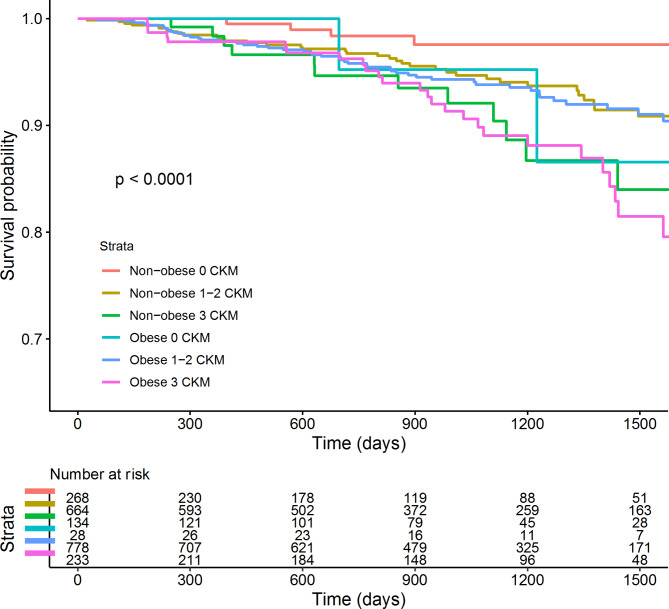
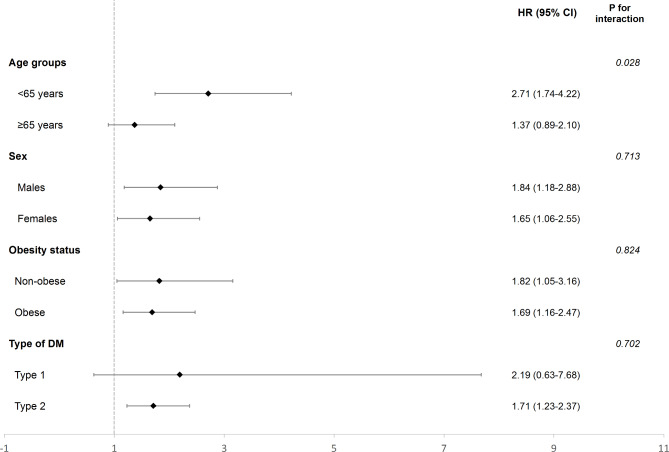
Results: 2105 people with DM were included [median age 60 (IQR 45-70), 48.8% females]. Both Group 1 and Group 6 were associated with a higher risk of events of the primary composite outcome (aHR 4.50, 95% CI 1.20-16.88; and aHR 3.78, 95% CI 1.06-13.47, respectively). On interaction analysis, in "extremely unhealthy" persons the impact of CKM comorbidities in determining the risk of adverse events was consistent in obese and non-obese ones (Pint=0.824), but more pronounced in individuals aged < 65 years compared to older adults (Pint= 0.028).
Conclusion: Both non-obese and obese people with DM and 3 associated CKM comorbidities represent an "extremely unhealthy" phenotype which are at the highest risk of CV adverse events. These results highlight the importance of risk stratification of people with DM for risk factor management utilising an interdisciplinary approach.
Keywords: Cardiovascular events; Comorbidities; Diabetes mellitus; Metabolically unhealthy; Obesity.
© 2024. The Author(s).
Conflict of interest statement
G.Y.H.L. is a consultant and speaker for BMS/Pfizer, Boehringer Ingelheim, Anthos and Daiichi-Sankyo. No fees are received personally. G.Y.H..L is a NIHR Senior Investigator and co-PI of the AFFIRMO project on multimorbidity in AF (grant agreement No 899871), TARGET project on digital twins for personalised management of atrial fibrillation and stroke (grant agreement No 101136244) and ARISTOTELES project on artificial intelligence for management of chronic long term conditions (grant agreement No 101080189), which are all funded by the EU’s Horizon Europe Research & Innovation programme. G.B. is Study Coordinator of ARISTOTELES (Applying ARtificial Intelligence to define clinical trajectorieS for personalized predicTiOn and early deTEction of comorbidity and muLtimorbidity pattErnS) Grant from Horizon Europe (HORIZON-HLTH-2022-STAYHLTH-01- Grant 101080189). G.B. received small speaker’s fee from Bayer, Boston, Boehringer Ingelheim, Brystol Myers Squibb, Janssen, and Sanofi. UA has received honoraria from Eli Lilly, Procter & Gamble, Viatris, Grunenthal and Sanofi for educational meetings and funding for attendance to an educational meeting from Diiachi Sankyo. UA has also received investigator-led funding by Procter & Gamble and is a council member of the Royal Society of Medicine's Vascular, Lipid & Metabolic Medicine Section. HK received remunerations/fees for activities on behalf of Sanofi-Aventis, Eli Lilly, Novo Nordisk, Servier, Astra-Zeneca, Boehringer-Ingelheim. JG received remunerations/fees for activities on behalf of Sanofi-Aventis, Eli Lilly, Novo Nordisk, Servier, Astra-Zeneca, Boehringer-Ingelheim, Bioton, Polfa Tarchomin, Medtronic, Roche, and Abbott. KN received remunerations/fees for activities on behalf of Sanofi-Aventis, Eli Lilly, Novo Nordisk, Servier, Astra-Zeneca, Boehringer-Ingelheim, Bioton, Polfa Tarchomin, Roche, and Abbott. All other authors report no disclosures.
Figures
References
-
- Leon BM, Maddox TM. Diabetes and cardiovascular disease: Epidemiology, biological mechanisms, treatment recommendations and future research. World J Diabetes. 2015;6(13):1246–58. 10.4239/wjd.v6.i13.1246. PubMed PMID: 26468341; PubMed Central PMCID: PMC4600176. 10.4239/wjd.v6.i13.1246 - DOI - PMC - PubMed
-
- Eeg-Olofsson K, Cederholm J, Nilsson PM, Zethelius B, Nunez L, Gudbjörnsdóttir S et al. Risk of cardiovascular disease and mortality in overweight and obese patients with type 2 diabetes: an observational study in 13,087 patients. Diabetologia. 2009;52(1):65–73. Epub 20081105. 10.1007/s00125-008-1190-x. PubMed PMID: 18985314. - PubMed
-
- Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM, et al. Management of hyperglycemia in type 2 diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–86. 10.2337/dci22-0034. PubMed PMID: 36148880; PubMed Central PMCID: PMC10008140. 10.2337/dci22-0034 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
