

Exploring the mortality and cardiovascular outcomes with SGLT-2 inhibitors in patients with T2DM at dialysis commencement: a health global federated network analysis
- PMID: 39227933
- PMCID: PMC11373240
- DOI: 10.1186/s12933-024-02424-7
Exploring the mortality and cardiovascular outcomes with SGLT-2 inhibitors in patients with T2DM at dialysis commencement: a health global federated network analysis
Abstract
Background: Sodium-glucose cotransporter 2 inhibitors (SGLT-2is) have demonstrated associations with lowering cardiovascular outcomes in patients with type 2 diabetes mellitus (T2DM). However, the impact of SGLT-2is on individuals at dialysis commencement remains unclear. The aim of this real-world study is to study the association between SGLT-2is and outcomes in patients with T2DM at dialysis commencement.
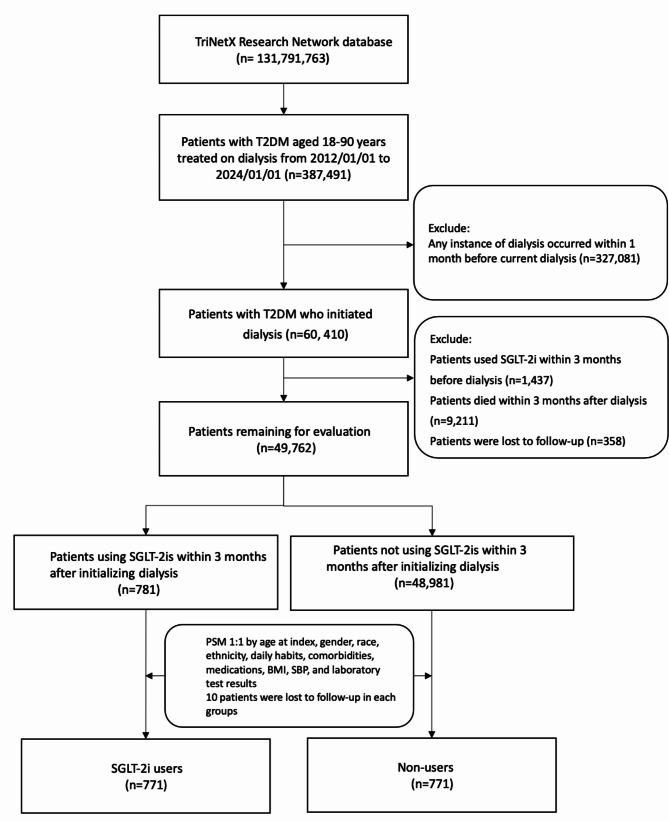
Methods: This is a retrospective cohort study of electronic health records (EHRs) of patients with T2DM from TriNetX Research Network database between January 1, 2012, and January 1, 2024. New-users using intention to treatment design was employed and propensity score matching was utilized to select the cohort. Clinical outcomes included major adverse cardiac events (MACE) and all-cause mortality. Safety outcomes using ICD-10 codes, ketoacidosis, urinary tract infection (UTI) or genital infection, dehydration, bone fracture, below-knee amputation, hypoglycemia, and achieving dialysis-free status at 90 days and 90-day readmission.
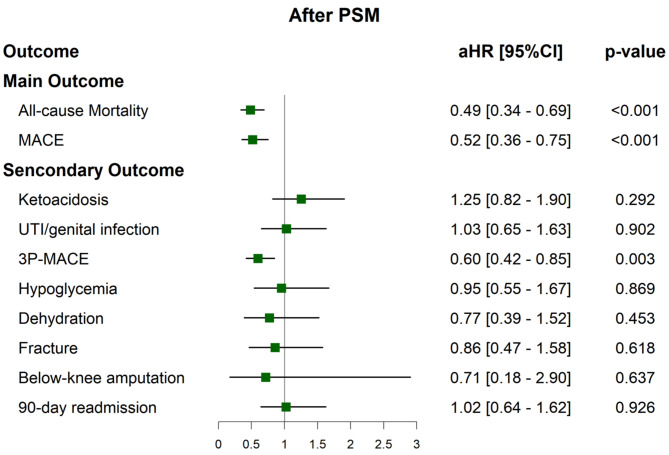
Results: Of 49,762 patients with T2DM who initiated dialysis for evaluation, a mere 1.57% of patients utilized SGLT-2is within 3 months after dialysis. 771 SGLT-2i users (age 63.3 ± 12.3 years, male 65.1%) were matched with 771 non-users (age 63.1 ± 12.9 years, male 65.8%). After a median follow-up of 2.0 (IQR 0.3-3.9) years, SGLT-2i users were associated with a lower risk of MACE (adjusted Hazard Ratio [aHR] = 0.52, p value < 0.001), all-cause mortality (aHR = 0.49, p < 0.001). SGLT-2i users were more likely to become dialysis-free 90 days after the index date (aHR = 0.49, p < 0.001). No significant differences were observed in the incidence of ketoacidosis, UTI or genital infection, hypoglycemia, dehydration, bone fractures, below-knee amputations, or 90-day readmissions.
Conclusions: Our findings indicated a lower incidence of all-cause mortality and MACE after long-term follow-up, along with a higher likelihood of achieving dialysis-free status at 90 days in SGLT-2i users. Importantly, they underscored the potential cardiovascular protection and safety of SGLT-2is use in T2DM patients at the onset of dialysis.
Keywords: Dialysis initiation; Major adverse cardiovascular events; Propensity score matching; Sodium-glucose cotransporter 2 inhibitors; Type 2 diabetes mellitus.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Comment in
-
Expanded response letter to "Hemodialysis dose and frequency should be considered in the subgroup analysis".Cardiovasc Diabetol. 2024 Nov 19;23(1):417. doi: 10.1186/s12933-024-02483-w. Cardiovasc Diabetol. 2024. PMID: 39563339 Free PMC article. No abstract available.
-
Hemodialysis dose and frequency should be considered in subgroup analysis.Cardiovasc Diabetol. 2024 Nov 19;23(1):416. doi: 10.1186/s12933-024-02482-x. Cardiovasc Diabetol. 2024. PMID: 39563369 Free PMC article.
References
-
- Federation ID. Diabetes and kidney disease: the latest data from the IDF diabetes atlas and the iCaReMe registry. 2024. Accessed 4 Aug 2024. https://diabetesatlas.org/atlas/diabetes-and-kidney-disease/
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
