

Robotic colorectal surgery training: Portsmouth perspective
- PMID: 39228198
- PMCID: PMC11375233
- DOI: 10.3393/ac.2024.00444.0063
Robotic colorectal surgery training: Portsmouth perspective
Abstract
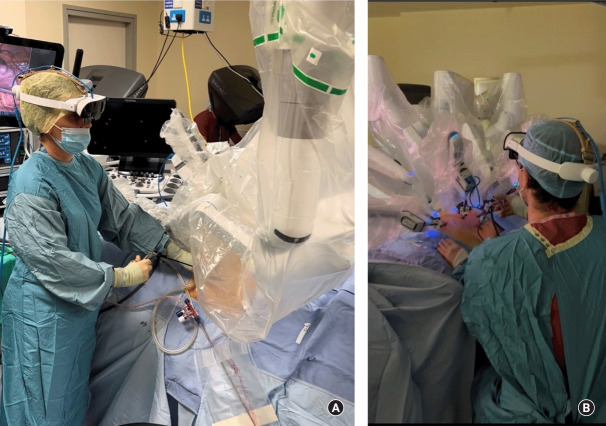
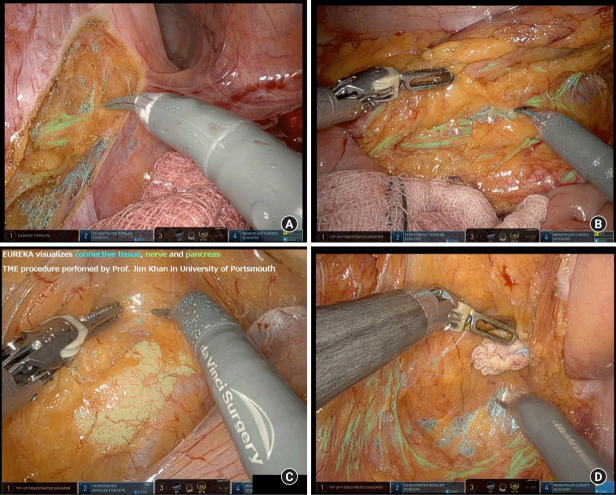
This study aims to discuss the principles and pillars of robotic colorectal surgery training and share the training pathway at Portsmouth Hospitals University NHS Trust. A narrative review is presented to discuss all the relevant and critical steps in robotic surgical training. Robotic training requires a stepwise approach, including theoretical knowledge, case observation, simulation, dry lab, wet lab, tutored programs, proctoring (in person or telementoring), procedure-specific training, and follow-up. Portsmouth Colorectal has an established robotic training model with a safe stepwise approach that has been demonstrated through perioperative and oncological results. Robotic surgery training should enable a trainee to use the robotic platform safely and effectively, minimize errors, and enhance performance with improved outcomes. Portsmouth Colorectal has provided such a stepwise training program since 2015 and continues to promote and augment safe robotic training in its field. Safe and efficient training programs are essential to upholding the optimal standard of care.
Keywords: Artificial intelligence; Colorectal surgery; Education; Robotics; Simulation training.
Conflict of interest statement
Jim S. Khan performs proctoring for Intuitive Surgical Inc and educational activity with Johnson & Johnson. No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- Ferrari D, Violante T, Novelli M, Starlinger PP, Smoot RL, Reisenauer JS, et al. The death of laparoscopy. Surg Endosc. 2024;38:2677–88. - PubMed
-
- Palagonia E, Mazzone E, De Naeyer G, D’Hondt F, Collins J, Wisz P, et al. The safety of urologic robotic surgery depends on the skills of the surgeon. World J Urol. 2020;38:1373–83. - PubMed
-
- O’Sullivan S, Leonard S, Holzinger A, Allen C, Battaglia F, Nevejans N, et al. Operational framework and training standard requirements for AI-empowered robotic surgery. Int J Med Robot. 2020;16:1–13. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
