

Outcome of Transcatheter Aortic Valve Replacement for Pure Native Aortic Regurgitation in Patients with Pulmonary Hypertension
- PMID: 39228503
- PMCID: PMC11366979
- DOI: 10.31083/j.rcm2508307
Outcome of Transcatheter Aortic Valve Replacement for Pure Native Aortic Regurgitation in Patients with Pulmonary Hypertension
Abstract
Background: In recent years, transcatheter aortic valve replacement (TAVR) has emerged as a pivotal treatment for pure native aortic regurgitation (PNAR). Given patients with severe aortic regurgitation (AR) are prone to suffer from pulmonary hypertension (PH), understanding TAVR's efficacy in this context is crucial. This study aims to explore the short-term prognosis of TAVR in PNAR patients with concurrent PH.
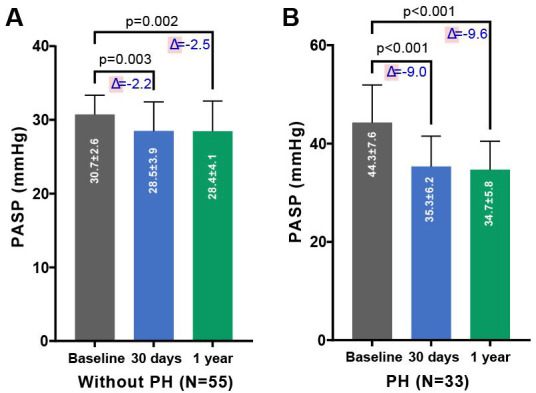
Methods: Patients with PNAR undergoing TAVR at Zhongshan Hospital, Affiliated with Fudan University, were enrolled between June 2018 to June 2023. They were categorized based on pulmonary artery systolic pressure (PASP) into groups with or without PH. The baseline characteristics, imaging records, and follow-up data were collected.
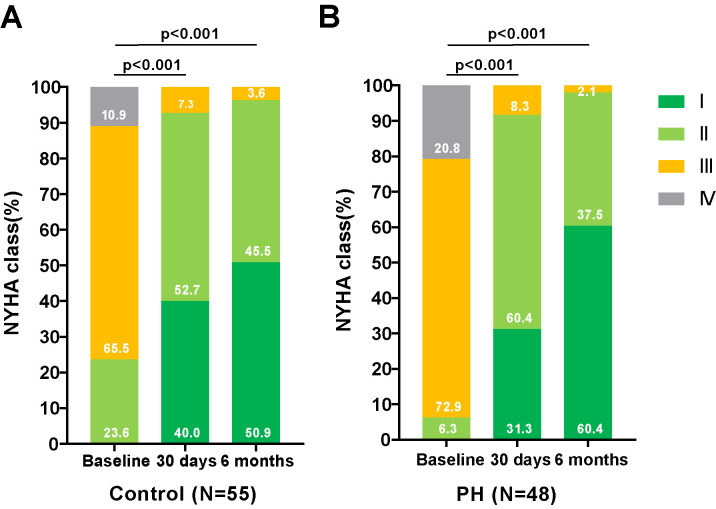
Results: Among the 103 patients recruited, 48 were afflicted with PH. In comparison to PNAR patients without PH, the PH group exhibited higher rates of renal dysfunction (10.4% vs. 0.0%, p = 0.014), increased Society of Thoracic Surgeons scores (6.4 1.9 vs. 4.7 1.6, p 0.001), and elevated Nterminal fragment of pro-brain natriuretic peptide (NT-proBNP). Transthoracic ultrasound examination revealed that patients with PH displayed lower left ventricular ejection fraction, larger left ventricle dimension, and more frequent moderate to severe tcuspid regurgitation (TR). Following TAVR, both groups experienced significant reductions in PASP, mitral regurgitation (MR) and TR. There were no significant differences in the incidence of postoperative adverse events in patients with or without PH.
Conclusions: We found TAVR to be a safe and effective treatment for patients with PNAR and PH, reducing the degree of aortic regurgitation and PH without increasing the risk of postoperative adverse events.
Keywords: pulmonary artery hypertension; pure native aortic regurgitation; retrospective; transcatheter aortic valve replacement.
Copyright: © 2024 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Pulmonary Hypertension in Patients With Severe Aortic Stenosis: Prognostic Impact After Transcatheter Aortic Valve Replacement: Pulmonary Hypertension in Patients Undergoing TAVR.JACC Cardiovasc Imaging. 2019 Apr;12(4):591-601. doi: 10.1016/j.jcmg.2018.02.015. Epub 2018 Apr 18. JACC Cardiovasc Imaging. 2019. PMID: 29680341
-
A study on correlation between preprocedural CT indexes and procedural success rate of transfemoral transcatheter aortic valve replacement with different self-expanding valves (VitaFlow or VenusA-Valve) in patients with pure native aortic regurgitation.Ann Transl Med. 2022 Jun;10(11):643. doi: 10.21037/atm-22-2588. Ann Transl Med. 2022. PMID: 35813316 Free PMC article.
-
Clinical characteristics of severe aortic stenosis patients combined with diabetes mellitus after transcatheter aortic valve replacement and short-term outcome.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022 Mar 28;47(3):309-318. doi: 10.11817/j.issn.1672-7347.2022.210357. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35545323 Free PMC article. Chinese, English.
-
Evaluating the effect of multivalvular disease on mortality after transcatheter aortic valve replacement for aortic stenosis: a meta-analysis and systematic review.Future Cardiol. 2022 Apr 29. doi: 10.2217/fca-2021-0061. Online ahead of print. Future Cardiol. 2022. PMID: 35485390 Review.
-
Transcatheter Aortic Valve Replacement for Pure Native Aortic Valve Regurgitation: A Systematic Review.Cardiology. 2018;141(3):132-140. doi: 10.1159/000491919. Epub 2018 Dec 5. Cardiology. 2018. PMID: 30517917
References
-
- Jilaihawi H, Chen M, Webb J, Himbert D, Ruiz CE, Rodés-Cabau J, et al. A Bicuspid Aortic Valve Imaging Classification for the TAVR Era. JACC. Cardiovascular Imaging . 2016;9:1145–1158. - PubMed
-
- Singh JP, Evans JC, Levy D, Larson MG, Freed LA, Fuller DL, et al. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study) The American Journal of Cardiology . 1999;83:897–902. - PubMed
-
- Markham R, Ghodsian M, Sharma R. TAVR in Patients with Pure Aortic Regurgitation: Ready to Use? Current Cardiology Reports . 2020;22:98. - PubMed
-
- Dujardin KS, Enriquez-Sarano M, Schaff HV, Bailey KR, Seward JB, Tajik AJ. Mortality and morbidity of aortic regurgitation in clinical practice. A long-term follow-up study. Circulation . 1999;99:1851–1857. - PubMed
-
- Tarasoutchi F, Grinberg M, Spina GS, Sampaio RO, Cardoso LUF, Rossi EG, et al. Ten-year clinical laboratory follow-up after application of a symptom-based therapeutic strategy to patients with severe chronic aortic regurgitation of predominant rheumatic etiology. Journal of the American College of Cardiology . 2003;41:1316–1324. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
