

This is a preprint.
Large-scale CSF proteome profiling identifies biomarkers for accurate diagnosis of Frontotemporal Dementia
- PMID: 39228745
- PMCID: PMC11370532
- DOI: 10.1101/2024.08.19.24312100
Large-scale CSF proteome profiling identifies biomarkers for accurate diagnosis of Frontotemporal Dementia
Update in
-
Large-scale CSF proteome profiling identifies biomarkers for accurate diagnosis of frontotemporal dementia.Mol Neurodegener. 2025 Aug 27;20(1):93. doi: 10.1186/s13024-025-00882-5. Mol Neurodegener. 2025. PMID: 40866991 Free PMC article.
Abstract
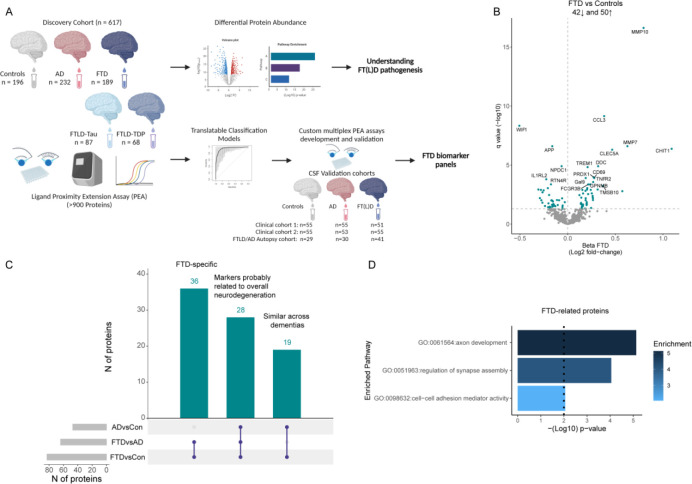
Diagnosis of Frontotemporal dementia (FTD) and the specific underlying neuropathologies (frontotemporal lobar degeneration; FTLD- Tau and FTLD-TDP) is challenging, and thus fluid biomarkers are needed to improve diagnostic accuracy. We used proximity extension assays to analyze 665 proteins in cerebrospinal fluid (CSF) samples from a multicenter cohort including patients with FTD (n = 189), Alzheimer's Disease dementia (AD; n = 232), and cognitively unimpaired individuals (n = 196). In a subset, FTLD neuropathology was determined based on phenotype or genotype (FTLD-Tau = 87 and FTLD-TDP = 68). Forty three proteins were differentially regulated in FTD compared to controls and AD, reflecting axon development, regulation of synapse assembly, and cell-cell adhesion mediator activity pathways. Classification analysis identified a 14- and 13-CSF protein panel that discriminated FTD from controls (AUC: 0.96) or AD (AUC: 0.91). Custom multiplex panels confirmed the highly accurate discrimination between FTD and controls (AUCs > 0.96) or AD (AUCs > 0.88) in three validation cohorts, including one with autopsy confirmation (AUCs > 0.90). Six proteins were differentially regulated between FTLD-TDP and FTLD-Tau, but no reproducible classification model could be generated (AUC: 0.80). Overall, this study introduces novel FTD-specific biomarker panels with potential use in diagnostic setting.
Keywords: Biomarkers; CSF; FTD; FTLD; Proteomics; TDP43; Tau.
Figures



References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources