

Excess long-term risk of adverse outcomes in heart failure patients with high and low levels of NT-proBNP: A 7-year follow-up study (NorthStar Trial)
- PMID: 39228977
- PMCID: PMC11368590
- DOI: 10.1016/j.ijcha.2024.101441
Excess long-term risk of adverse outcomes in heart failure patients with high and low levels of NT-proBNP: A 7-year follow-up study (NorthStar Trial)
Abstract
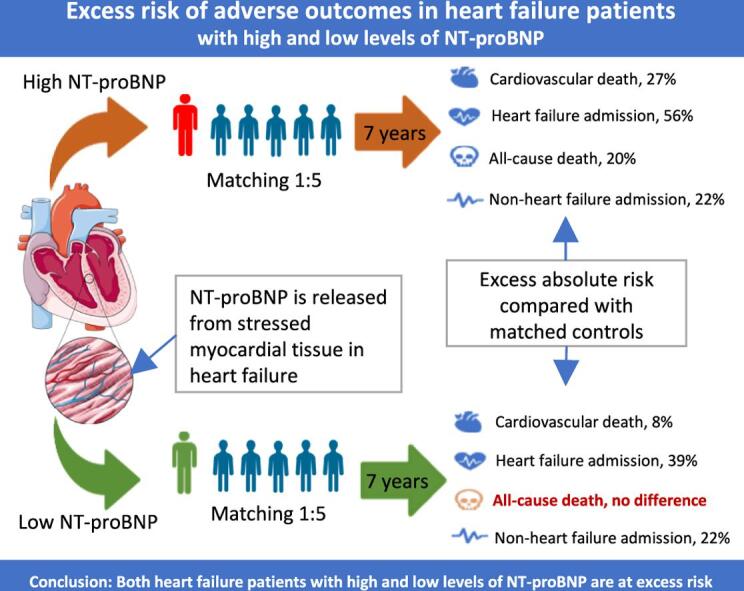
Background: This study investigated excess risk in patients with heart failure with reduced left ventricular ejection fraction (HFrEF) with or without elevated levels of NT-proBNP (N-terminal pro-brain natriuretic peptide).
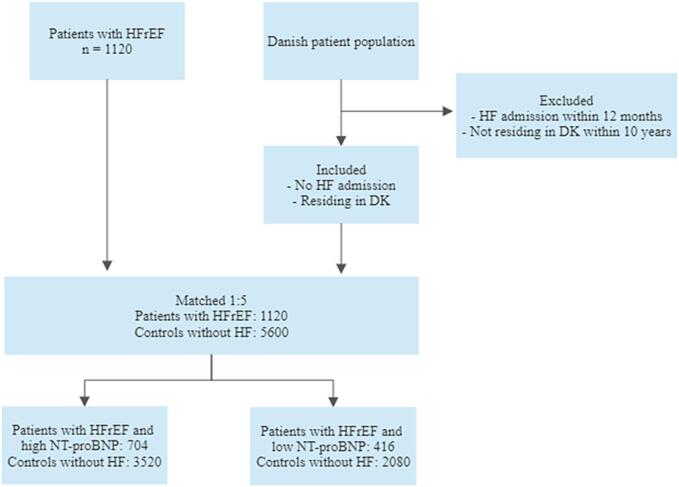
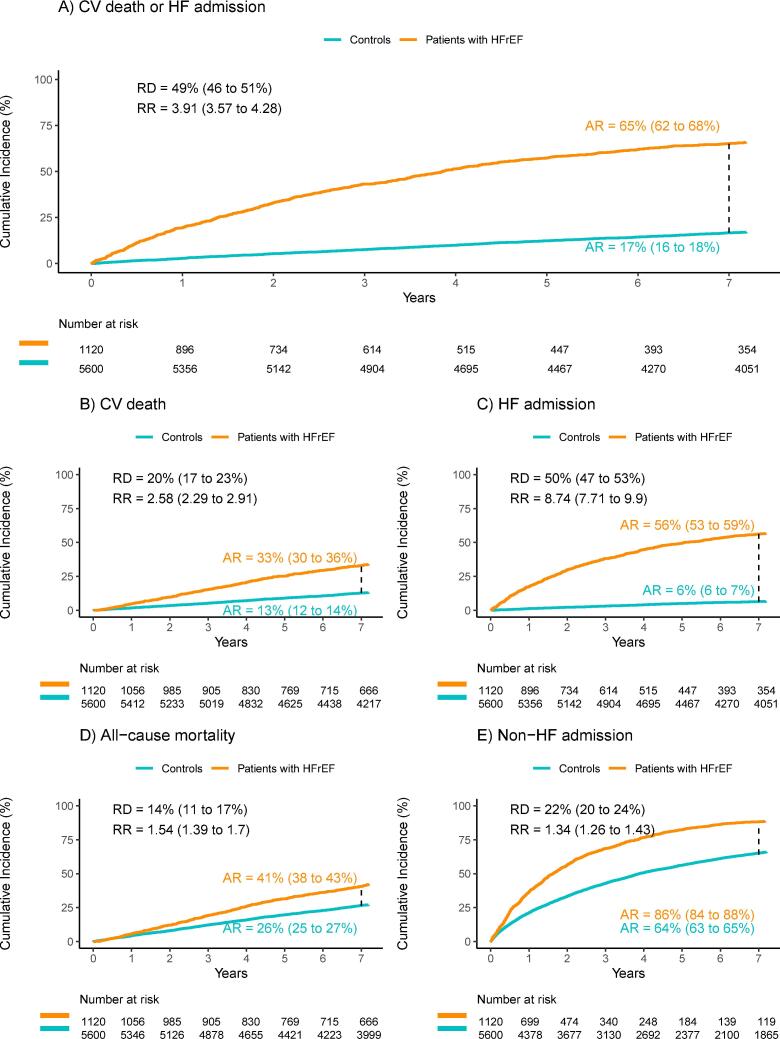
Methods: Patients with HFrEF from the NorthStar cohort (n = 1120) were matched on age, sex, and presence of AF (atrial fibrillation/flutter) to five controls without HFrEF from The Danish National Patient Registries. Patients were compared with controls before and after stratification according to baseline NT-proBNP levels, with cutoffs defined as </≥ 600 pg/ml in patients with sinus rhythm and </≥ 900 pg/ml in patients with AF. The primary composite endpoint was a 7-year risk of cardiovascular death or HF admission.
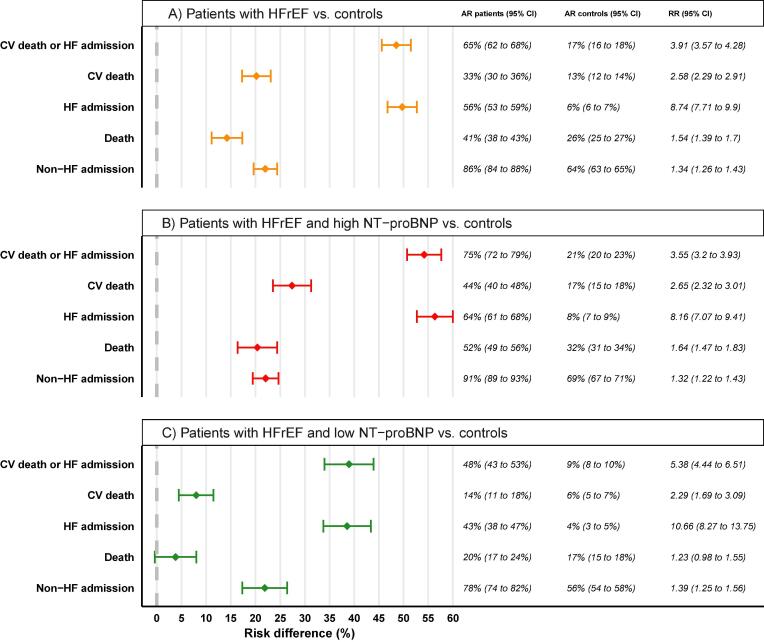
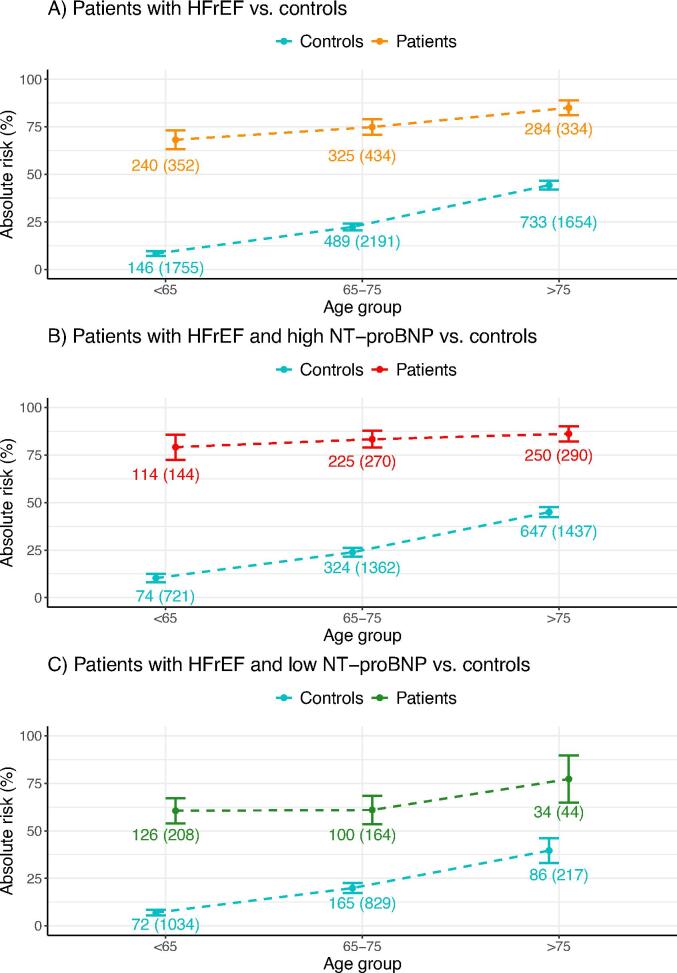
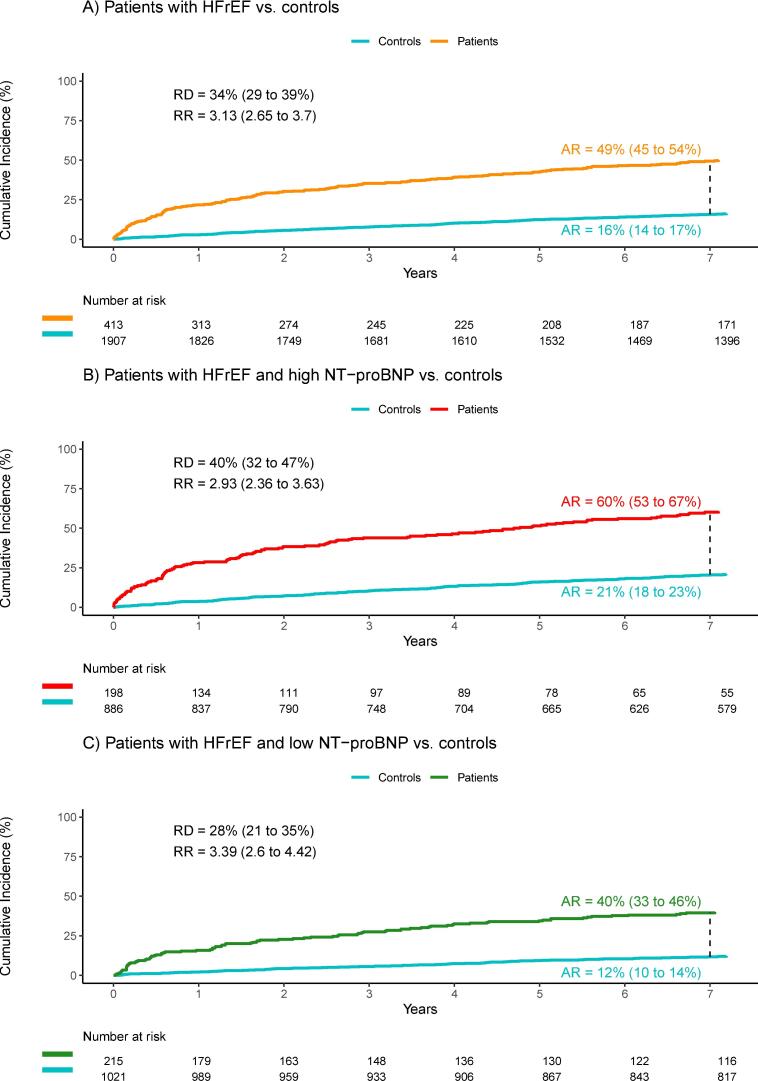
Results: In the HFrEF cohort, 704 patients had high NT-proBNP (median age, 73; mean left ventricular ejection fraction (LVEF), 33%). 416 patients had low NT-proBNP (median age, 65; LVEF, 30%). Patients from both groups were in NYHA class I-III. The primary endpoint occurred in 531 patients (75.4%) with HFrEF and elevated NT-proBNP, and 748 controls (21.3%) (risk difference, 54.2%; 95% confidence interval (CI) 50.7-57.6%). In comparison, it occurred in 199 patients (47.9%) with HFrEF and without elevated NT-proBNP, and 185 controls (8,9%) (risk difference, 38.9%; 95% CI 34.0-43.9%). Risk differences for all secondary endpoints were significant, except for overall mortality in the low NT-proBNP group (risk difference, 3.8%; 95% CI, -0.4-8.0%).
Conclusion: This study identified a significant excess risk in patients with HFrEF across various endpoints, which persisted after stratification into high and low levels of NT-proBNP.
Keywords: Excess risk; Heart failure; NT-proBNP; NorthStar.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- McMurray J.J., Packer M., Desai A.S., et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014;371(11):993–1004. - PubMed
-
- McMurray J.J.V., Solomon S.D., Inzucchi S.E., et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N. Engl. J. Med. 2019;381(21):1995–2008. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
