

Twelve-month results from a randomized controlled trial comparing differential target multiplexed spinal cord stimulation and conventional spinal cord stimulation in subjects with chronic refractory axial low back pain not eligible for spine surgery
- PMID: 39229594
- PMCID: PMC11369449
- DOI: 10.1016/j.xnsj.2024.100528
Twelve-month results from a randomized controlled trial comparing differential target multiplexed spinal cord stimulation and conventional spinal cord stimulation in subjects with chronic refractory axial low back pain not eligible for spine surgery
Abstract
Background: Successful treatments for intractable chronic low back pain (CLBP) in patients who are not eligible for surgical interventions are scarce. The superior efficacy of differential target multiplexed spinal cord stimulation (DTM SCS) to conventional SCS (Conv-SCS) on the treatment of CLBP in patients with persistent spinal pain syndrome (PSPS) who have failed surgical interventions (PSPS-T2) motivated the evaluation of DTM SCS versus Conv-SCS on PSPS patients who are non-surgical candidates (PSPS-T1).
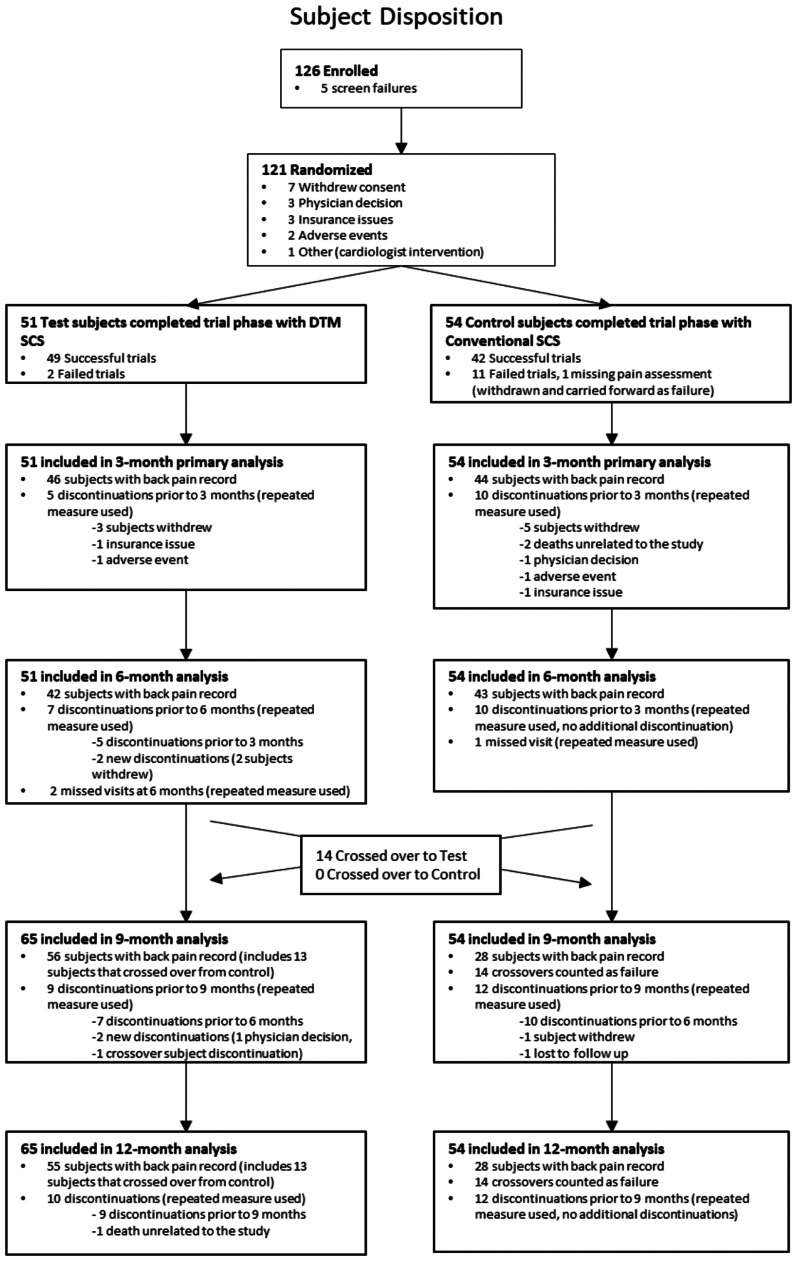
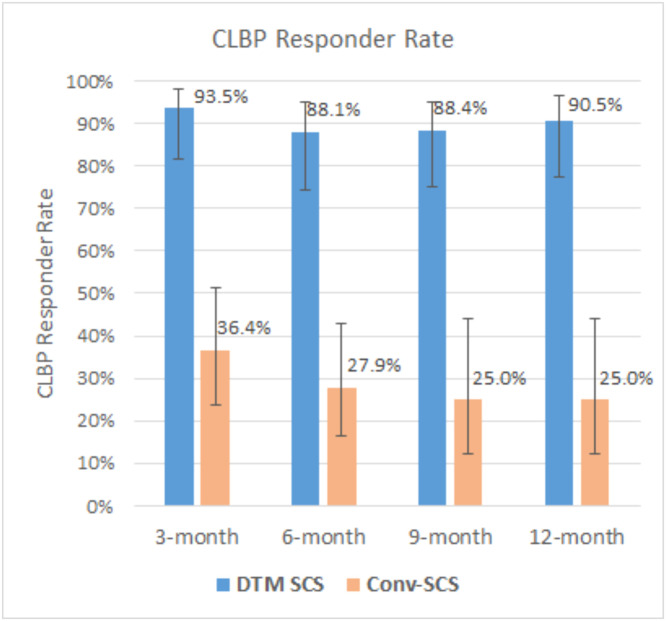
Methods: This is a prospective, open label, crossover, post-market randomized controlled trial in 20 centers across the United States. Eligible patients were randomized to either DTM SCS or Conv-SCS in a 1:1 ratio. Primary endpoint was CLBP responder rate (percentage of subjects with ≥50% CLBP relief) at 3-month in randomized subjects who completed trialing (modified intention-to-treat population). Patients were followed up to 12 months. Secondary endpoints included change of CLBP and leg pain, responder rates, changes in disability, quality of life, patient satisfaction and global impression of change, and safety profile. An optional crossover was available at 6-month to all patients.
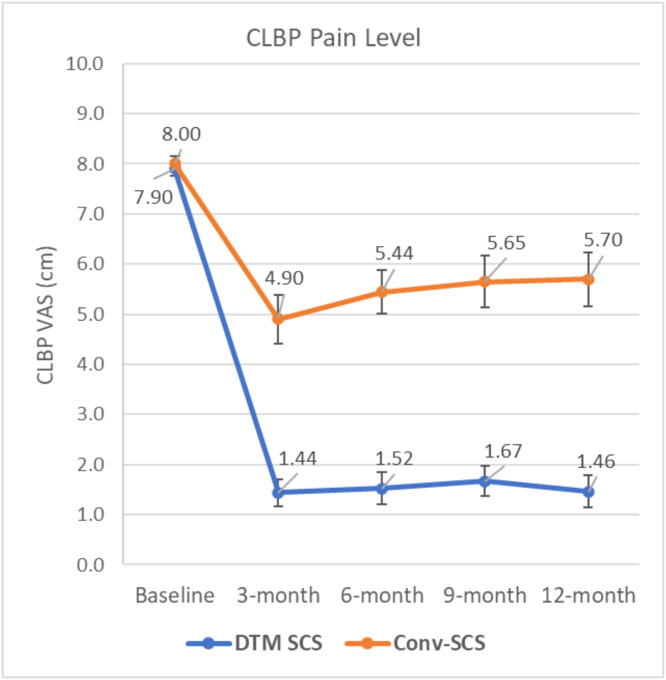
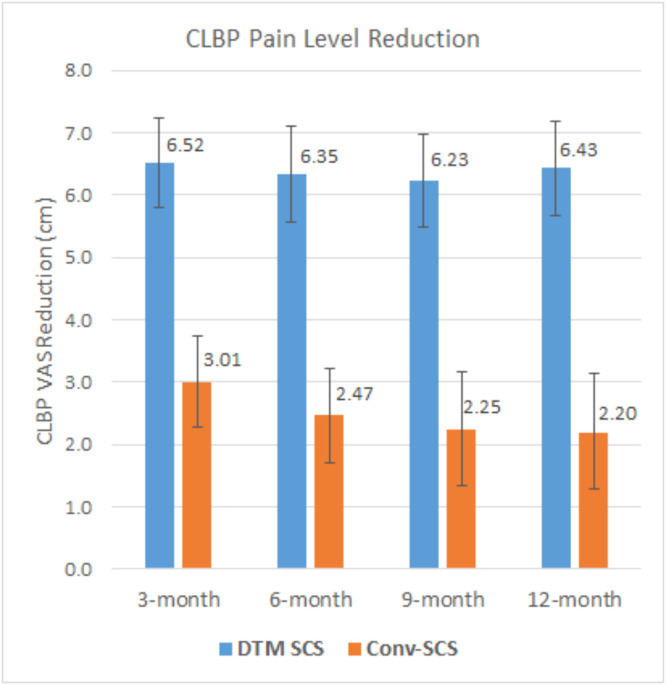
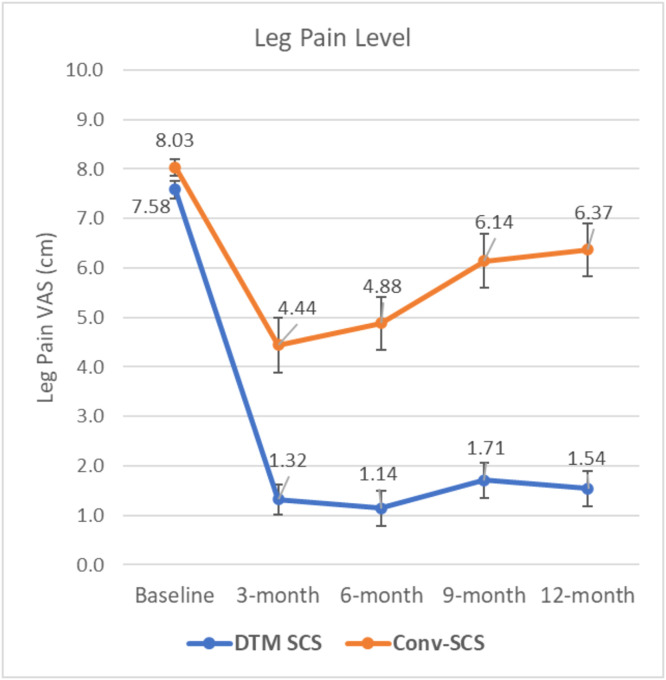
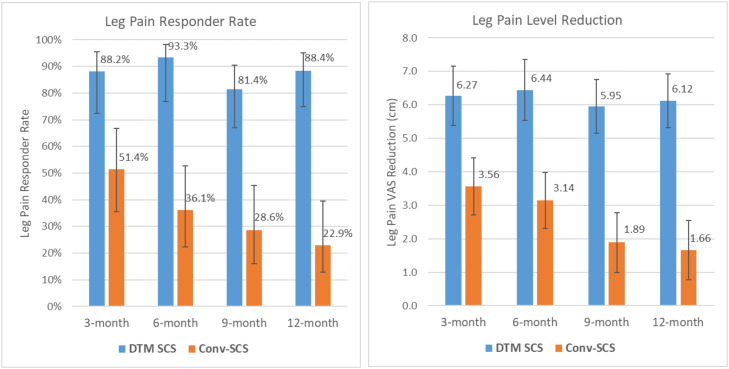
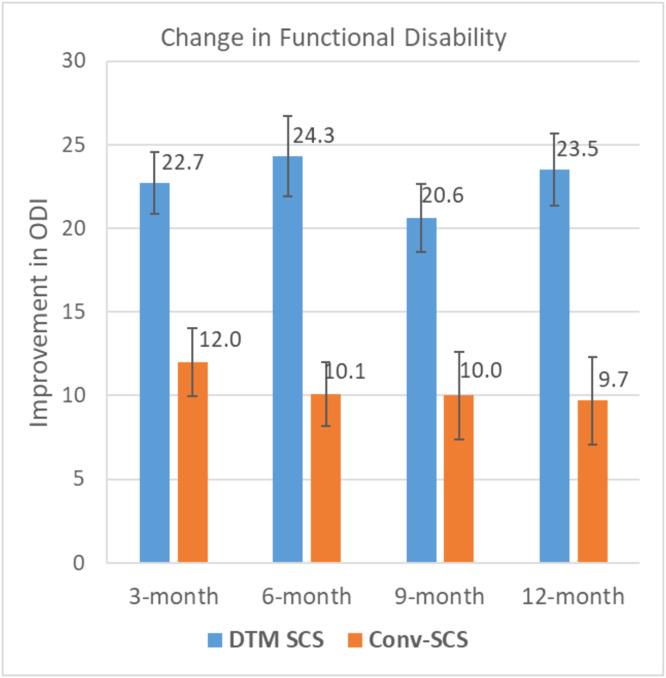
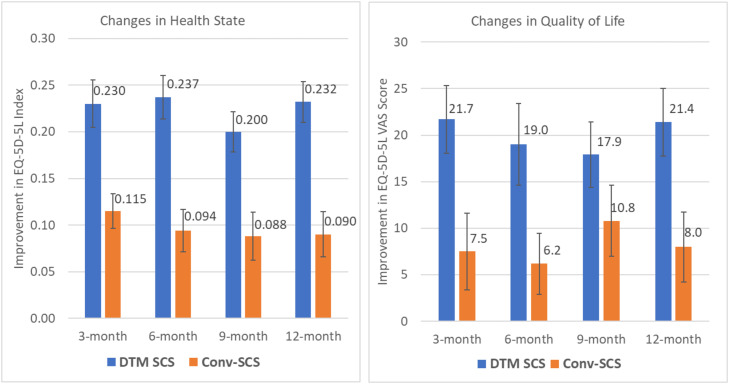
Results: About 121 PSPS-T1 subjects with CLBP and leg pain mostly associated with degenerative disc disease and radiculopathy and who were not eligible for spine surgery were randomized. CLBP responder rate with DTM SCS (93.5%) was superior to Conv-SCS (36.4%) at the primary endpoint. Superior CLBP responder rates (88.1%-90.5%) were obtained with DTM SCS at all other timepoints. Mean CLBP reduction with DTM SCS (6.52 cm) was superior to that with Conv-SCS (3.01 cm) at the primary endpoint. Similar CLBP reductions (6.23-6.43 cm) were obtained with DTM SCS at other timepoints. DTM SCS provided significantly better leg pain reduction and responder rate, improvement of disability and quality of life, and better patient satisfaction and global impression of change. 90.9% of Conv-SCS subjects who crossed over were CLBP responders at completion of the study. Similar safety profiles were observed between the two groups.
Conclusion: DTM SCS for chronic CLBP in nonsurgical candidates is superior to Conv-SCS. Improvements were sustained and provided significant benefits on the management of these patients.
Keywords: Conventional SCS; Differential target multiplexed SCS; Nonsurgical candidates; Persistent spinal pain syndrome type 1; Randomized controlled trial; Spinal cord stimulation.
© 2024 The Author(s).
Conflict of interest statement
One or more of the authors declare financial or professional relationships on ICMJE-NASSJ disclosure forms.
Figures
References
-
- Deer TR, Mekhail N, Provenzano D, et al. Neuromodulation appropriateness consensus committee. The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: the neuromodulation appropriateness consensus committee. Neuromodulation. 2014;17(6):515–550. doi: 10.1111/ner.12208. - DOI - PubMed
-
- Kapural L, Yu C, Doust MW, et al. Novel 10-kHz high-frequency therapy (HF10 therapy) is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: The SENZA-RCT randomized controlled trial. Anesthesiology. 2015;123(4):851–860. doi: 10.1097/ALN.0000000000000774. - DOI - PubMed
LinkOut - more resources
Full Text Sources
