

Mechanical ventilation settings during weaning from venovenous extracorporeal membrane oxygenation
- PMID: 39230734
- PMCID: PMC11374948
- DOI: 10.1186/s13613-024-01359-2
Mechanical ventilation settings during weaning from venovenous extracorporeal membrane oxygenation
Abstract
Background: The optimal timing of weaning from venovenous extracorporeal membrane oxygenation (VV ECMO) and its modalities have been rarely studied.
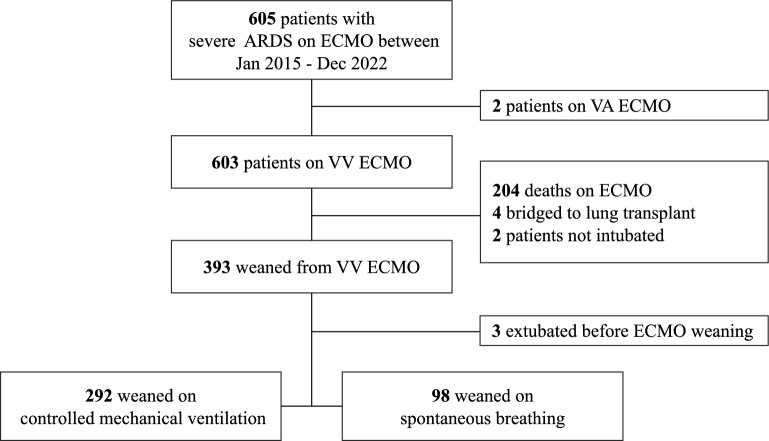
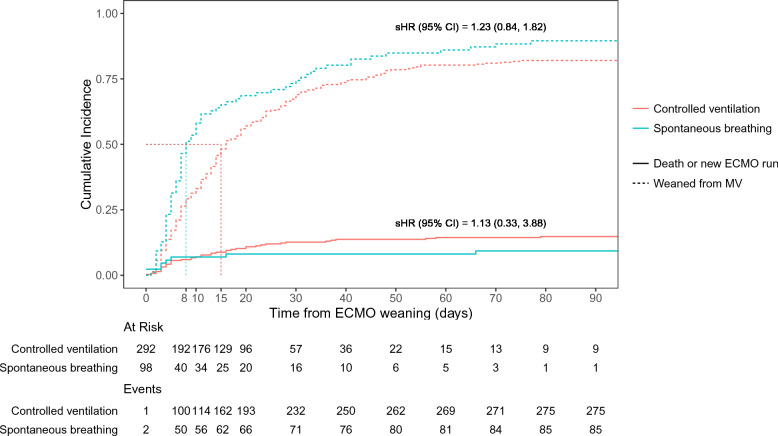
Methods: Retrospective, multicenter cohort study over 7 years in two tertiary ICUs, high-volume ECMO centers in France and Italy. Patients with ARDS on ECMO and successfully weaned from VV ECMO were classified based on their mechanical ventilation modality during the sweep gas-off trial (SGOT) with either controlled mechanical ventilation or spontaneous breathing (i.e. pressure support ventilation). The primary endpoint was the time to successful weaning from mechanical ventilation within 90 days post-ECMO weaning.
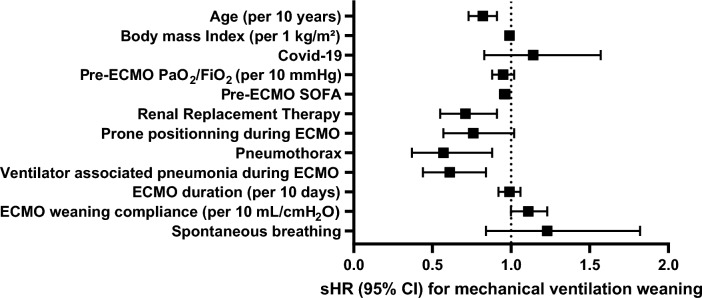
Results: 292 adult patients with severe ARDS were weaned from controlled ventilation, and 101 were on spontaneous breathing during SGOT. The 90-day probability of successful weaning from mechanical ventilation was not significantly different between the two groups (sHR [95% CI], 1.23 [0.84-1.82]). ECMO-related complications were not statistically different between patients receiving these two mechanical ventilation strategies. After adjusting for covariates, older age, higher pre-ECMO sequential organ failure assessment score, pneumothorax, ventilator-associated pneumonia, and renal replacement therapy, but not mechanical ventilation modalities during SGOT, were independently associated with a lower probability of successful weaning from mechanical ventilation after ECMO weaning.
Conclusions: Time to successful weaning from mechanical ventilation within 90 days post-ECMO was not associated with the mechanical ventilation strategy used during SGOT. Further research is needed to assess the optimal ventilation strategy during weaning off VV ECMO and its impact on short- and long-term outcomes.
Keywords: Acute respiratory distress syndrome; Extracorporeal membrane oxygenation; Mechanical ventilation; Spontaneous breathing; Weaning.
© 2024. The Author(s).
Conflict of interest statement
Matthieu Schmidt reports lecture fees from Getinge, Dräger, Baxter, and Fresenius Medical Care outside the submitted work. Alain Combes reports grants from Getinge, and personal fees from Getinge, Baxter, and Xenios outside the submitted work. The other authors declare that they have no conflict of interest.
Figures
References
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. The Lancet. 2009;374:1351–63. 10.1016/S0140-6736(09)61069-2 - DOI - PubMed
-
- Goligher EC, Tomlinson G, Hajage D, Wijeysundera DN, Fan E, Jüni P, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome and posterior probability of mortality benefit in a post hoc Bayesian analysis of a randomized clinical trial. JAMA. 2018;320:2251. 10.1001/jama.2018.14276 - DOI - PubMed
LinkOut - more resources
Full Text Sources
