

Mycoplasma hominis as Cause of Extragenital Infection in Patients with Hypogammaglobulinemia: Report of 2 Cases and Literature Review
- PMID: 39230828
- PMCID: PMC11416451
- DOI: 10.1007/s40121-024-01035-9
Mycoplasma hominis as Cause of Extragenital Infection in Patients with Hypogammaglobulinemia: Report of 2 Cases and Literature Review
Abstract
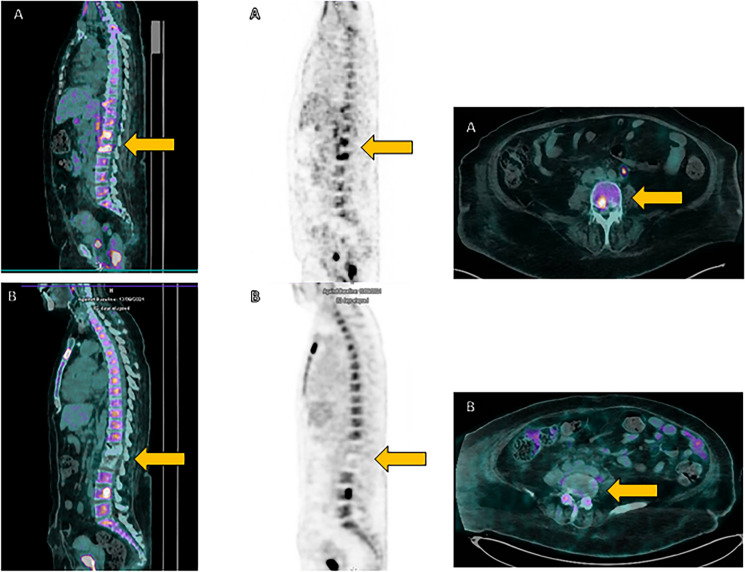
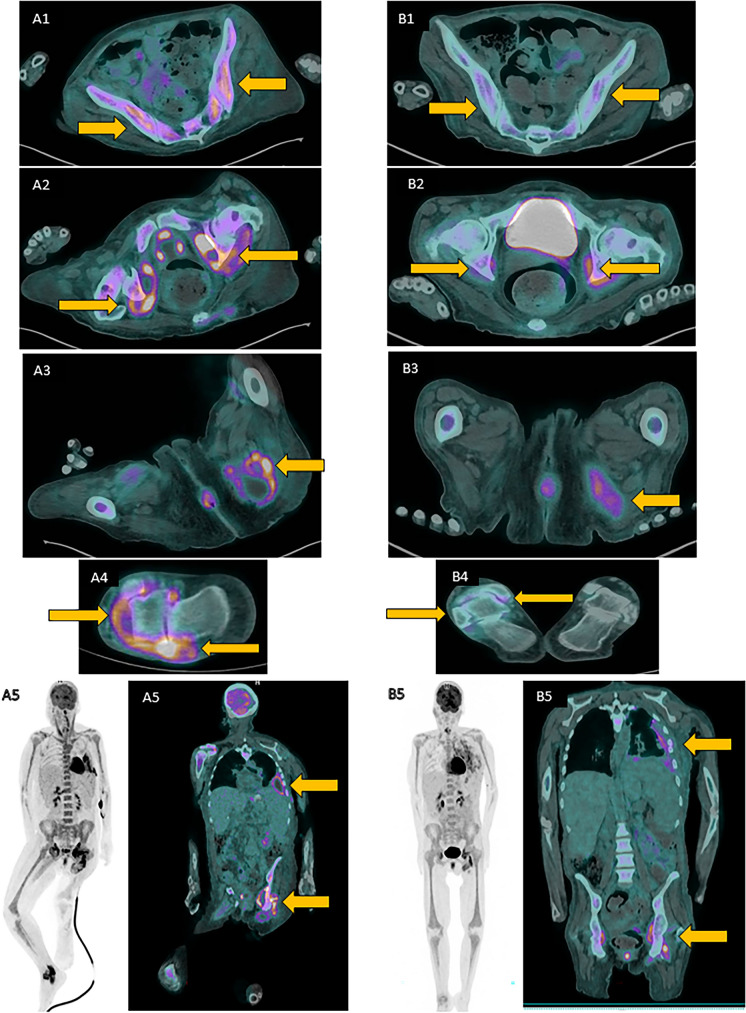
Mycoplasma hominis can be a part of human urogenital tract microbiome, and it is a frequent cause of urogenital infections. In rare cases, it can also cause extragenital infections, especially in immunocompromised patients. In this case series, we report two cases and provide a literature review of extragenital infections caused by M. hominis in patients with hypogammaglobulinemia. Patient 1 was a 61-year-old woman with diffuse large B-cell lymphoma who, after rituximab-containing chemotherapy and CAR-T therapy, developed M. hominis spondylodiscitis. Patient 2 was a 50-year-old woman with congenital hypogammaglobulinemia who developed disseminated M. hominis infection involving pleura, muscles, and right ankle. Antibiotic therapy with levofloxacin and doxycycline for 10 weeks in patient 1 and with levofloxacin alone for 6 weeks in patient 2 led to infection resolution. The literature review identified 14 additional cases reporting M. hominis extragenital infection in patients with hypogammaglobulinemia. M. hominis should also be suspected as an etiological agent of extragenital infection in patients with B-cell immunodeficiency with a clinical picture of persistent, standard-culture negative infection, particularly with arthritis or abscess formation. Even if M. hominis can grow on standard bacterial medium, in suspected cases molecular methods should be promptly used for correct diagnostic work-up and successful therapy.
Keywords: Mycoplasma hominis; Extragenital infection; Hypogammaglobulinemia.
© 2024. The Author(s).
Conflict of interest statement
Matteo Bassetti received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events of Angelini, Cidara, Gilead, Menarini, MSD, Pfizer, Shionogi, Multipharma. MB participated on a Data Safety Monitoring Board or Advisory Board with Angelini, Cidara, Gilead, Menarini, MSD, Pfizer, Shionogi, Multipharma. Malgorzata Mikulska is an Editorial Board member of Infectious Diseases and Therapy and was not involved in the selection of peer reviewers for the manuscript nor any of the subsequent editorial decisions. Chiara Russo, Emanuele Delfino, Federica Toscanini, Laura Mezzogori, Riccardo Schiavoni, Claudia Bartalucci, Emanuele Angelucci, Giulia Bartalucci, Massimilano Gambella, Anna Maria Crea, Paolo Morici, Francesca Crea, Silvia Chiola, Silvia Daniela Morbelli, and Anna Marchese have no conflicts of interest to declare.
Figures
References
-
- Ahmed J, et al. Mycoplasma hominis: an under recognized pathogen. Indian J Med Microbiol. 2021;39(1):88–97. - PubMed
-
- Pettersson B, et al. Updated phylogenetic description of the Mycoplasma hominis cluster (Weisburg et al. 1989) based on 16S rDNA sequences. Int J Syst Evol Microbiol. 2000;50 Pt 1:291–301. - PubMed
-
- Taylor-Robinson D. Mollicutes in vaginal microbiology: Mycoplasma hominis, Ureaplasma urealyticum, Ureaplasma parvum and Mycoplasma genitalium. Res Microbiol. 2017;168(9–10):875–81. - PubMed
-
- Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases, vol. 2. 9th ed. Amsterdam: Elsevier; 2019.
-
- Horner P, et al. Should we be testing for urogenital Mycoplasma hominis, Ureaplasma parvum and Ureaplasma urealyticum in men and women?—a position statement from the European STI Guidelines Editorial Board. J Eur Acad Dermatol Venereol. 2018;32(11):1845–51. - PubMed
LinkOut - more resources
Full Text Sources
