

Early Circulating Tumor DNA Shedding Kinetics for Prediction of Platinum Sensitivity in Patients With Small Cell Lung Cancer
- PMID: 39231375
- PMCID: PMC11376985
- DOI: 10.1200/PO.24.00216
Early Circulating Tumor DNA Shedding Kinetics for Prediction of Platinum Sensitivity in Patients With Small Cell Lung Cancer
Abstract
Purpose: Small cell lung cancer (SCLC) is characterized by rapid progression after platinum resistance. Circulating tumor (ctDNA) dynamics early in treatment may help determine platinum sensitivity.
Materials and methods: Serial plasma samples were collected from patients receiving platinum-based chemotherapy for SCLC on the first 3 days of cycle one and on the first days of subsequent cycles with paired samples collected both before and again after infusions. Tumor-informed plasma analysis was carried out using CAncer Personalized Profiling by deep Sequencing (CAPP-Seq). The mean variant allele frequency (VAF) of all pretreatment mutations was tracked in subsequent blood draws and correlated with radiologic response.
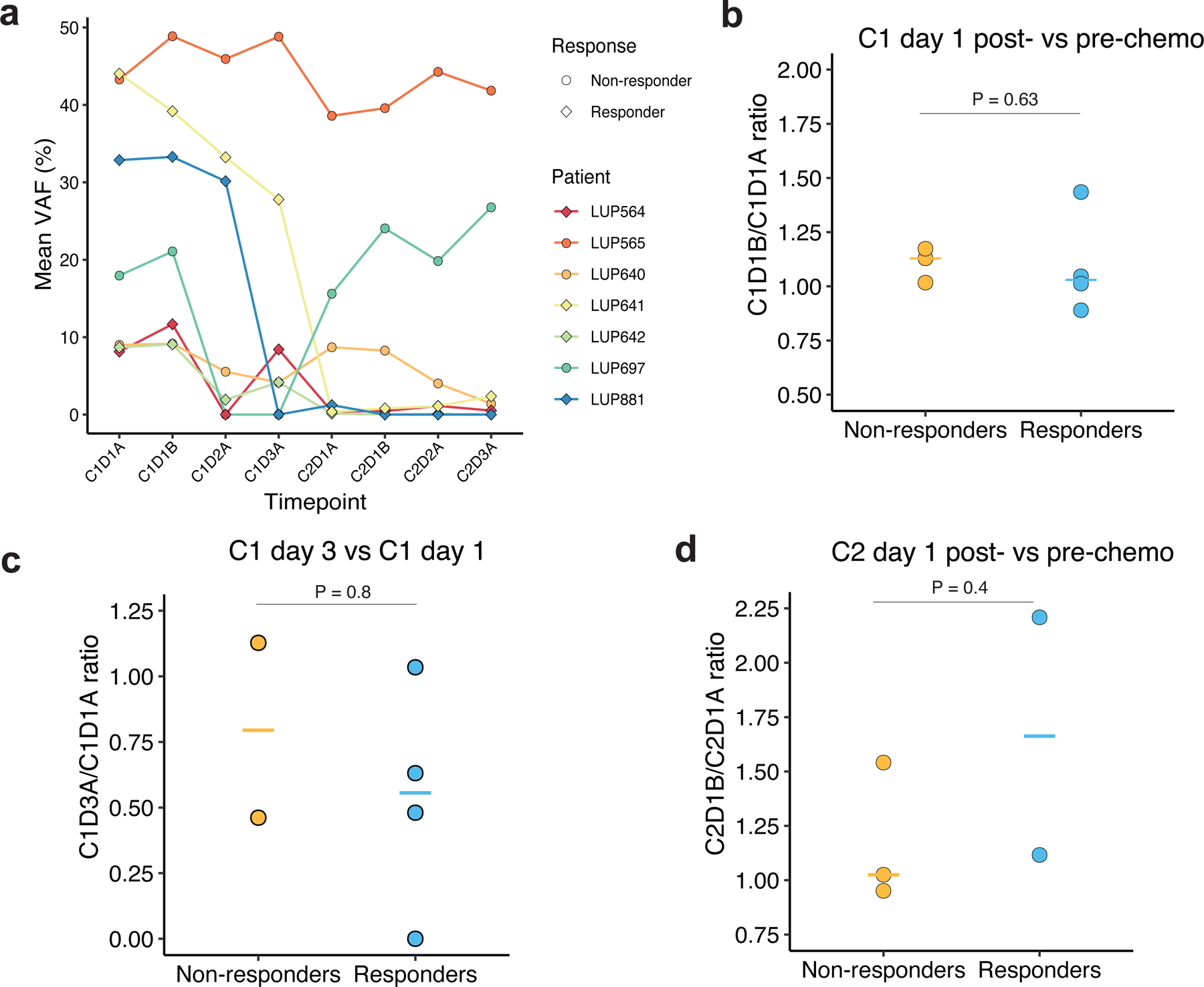
Results: ctDNA kinetics were assessed in 122 samples from 21 patients. Pretreatment VAF did not differ significantly between patients who did and did not respond to chemotherapy (mean 22.5% v 4.6%, P = .17). A slight increase in ctDNA on cycle 1, day 1 immediately post-treatment was seen in six of the seven patients with available draws (fold change from baseline: 1.01-1.44), half of whom achieved a response. All patients who responded had a >2-fold decrease in mean VAF on cycle 2 day 1 (C2D1). Progression-free survival (PFS) and overall survival (OS) were significantly longer in patients with a >2-fold decrease in mean VAF after one treatment cycle (6.8 v 2.6 months, log-rank P = .0004 and 21.7 v 6.4 months, log rank P = .04, respectively).
Conclusion: A >2-fold decrease in ctDNA concentration was observed by C2D1 in all patients who were sensitive to platinum-based therapy and was associated with longer PFS and OS.
Conflict of interest statement
Conflict of interest statement:
Y.R.M.-G. reports travel, accommodation, and expenses from AstraZeneca and Loxo Oncology/ Eli Lilly. She acknowledges honoraria from Virology Education and Projects in Knowledge (for a CME program funded by an educational grant from Amgen). She has been on an advisory board for Revolution Medicines. She acknowledges associated research funding to the institution from Mirati Therapeutics, Bristol Myers Squibb, Loxo Oncology at Eli Lilly, Elucida Oncology, Taiho Oncology, Hengrui USA, Ltd/ Jiangsu Hengrui Pharmaceuticals, Luzsana Biotechnology, Endeavor Biomedicines, and AbbVie. She is an employee of Memorial Sloan Kettering Cancer Center, which has an institutional interest in Elucida. She acknowledges royalties from Rutgers University Press and Wolters Kluwer. She acknowledges food/beverages from Endeavor Biomedicines. Y.R. Murciano-Goroff acknowledges receipt of training through an institutional K30 grant from the NIH (CTSA UL1TR00457). She has received funding from a Kristina M. Day Young Investigator Award from Conquer Cancer, the ASCO Foundation, endowed by Dr. Charles M. Baum and Carol A. Baum. She is also funded by the Fiona and Stanley Druckenmiller Center for Lung Cancer Research, the Andrew Sabin Family Foundation, the Society for MSK, the Squeri Grant for Drug Development, and a Paul Calabresi Career Development Award for Clinical Oncology (NIH/NCI K12 CA184746) as well as through NIH/NCI R01 CA279264.
Figures





References
-
- Govindan R, Page N, Morgensztern D, et al. : Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol 24:4539–44, 2006 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
