

Diagnostic Value of Inter-Eye Difference Metrics on OCT for Myelin Oligodendrocyte Glycoprotein Antibody-Associated Optic Neuritis
- PMID: 39231384
- PMCID: PMC11379125
- DOI: 10.1212/NXI.0000000000200291
Diagnostic Value of Inter-Eye Difference Metrics on OCT for Myelin Oligodendrocyte Glycoprotein Antibody-Associated Optic Neuritis
Abstract
Background and objectives: The 2022 International Consortium for Optic Neuritis diagnostic criteria for optic neuritis (ON) include optical coherence tomography (OCT). The diagnostic value of intereye difference (IED) metrics is high for ON in patients with multiple sclerosis and aquaporin-4 antibody seropositive neuromyelitis optica spectrum disorders, but unknown in myelin oligodendrocyte glycoprotein antibody-associated ON (MOG-ON).
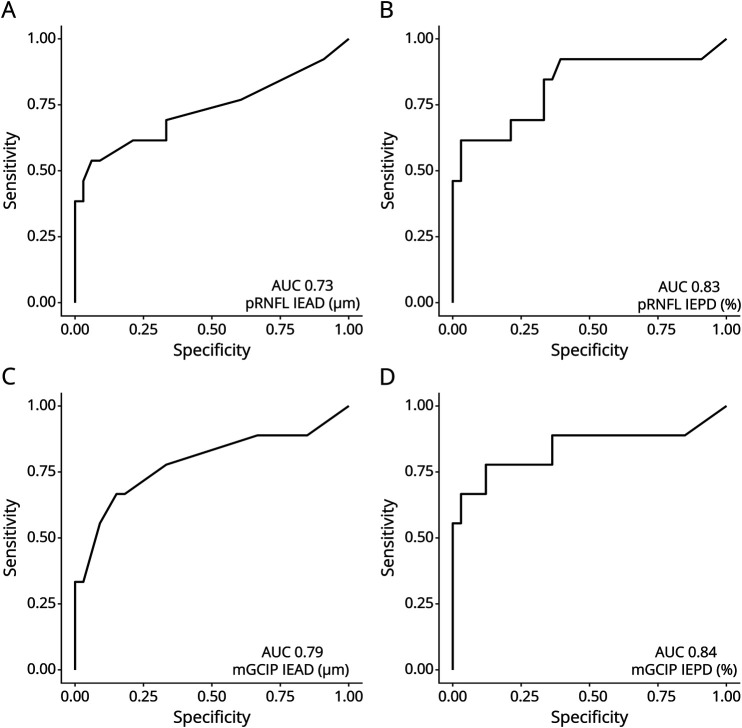
Methods: A multicenter validation study was conducted on the published IED cutoff values (>4% or >4 μm in the macular ganglion cell and inner plexiform layer [mGCIP] or >5% or >5 μm in the peripapillary retinal nerve fiber layer [pRNFL]) in individuals with MOG-ON and age-matched and sex-matched healthy controls (HCs). Structural data were acquired with Spectralis spectral-domain OCT >6 months after ON. We calculated sensitivity, specificity, and receiver operating characteristics for both intereye percentage (IEPD) and absolute difference (IEAD).
Results: A total of 66 individuals were included (MOG-ON N = 33; HCs N = 33). ON was unilateral in 20 and bilateral in 13 subjects. In the pooled analysis, the mGCIP IEPD was most sensitive (92%), followed by the mGCIP IEAD (88%) and pRNFL (84%). The same pattern was found for the specificity (mGCIP IEPD 82%, IEAD 82%; pRNFL IEPD 82%, IEAD 79%).In subgroup analyses, the diagnostic sensitivity was higher in subjects with unilateral ON (>99% for all metrics) compared with bilateral ON (61%-78%).
Discussion: In individuals with MOG-ON, the diagnostic accuracy of OCT-based IED metrics for ON was high, especially of mGCIP IEPD.
Classification of evidence: This study provides Class III evidence that the intereye difference on OCT can distinguish between those with MOG and normal controls.
Conflict of interest statement
A. Petzold received grant support for remyelination trials in multiple sclerosis to the Amsterdam University Medicam Centre, Department of Neurology, MS Centre (RESTORE trial) and UCL, London RECOVER trial, Fight for Sight (nimodipine in optic neuritis trial), royalties or licenses from Up-to-Date (Wolters Kluver) on a book chapter, speaker fees for the Heidelberg Academy, participation on Advisory Board SC Zeiss OCTA Angi-Network, SC Novartis OCTiMS study, leadership roles for governing board IMSVISUAL (until DEC-2022), chairman ERN-EYE Neuro-ophthalmology (until OCT-2020), board member of National Dutch Neuro-ophthalmology Association, equipment: OCTA from Zeiss (Plex Elite), medical writing: Support from Novartis for manuscript doi: 10.1002/acn3.51473. F.C. Oertel reports past research funding by the American Academy of Neurology, the National Multiple Sclerosis Society (US) and the German Association of Neurology (DGN); current research support by the Hertie Foundation for Excellence in Clinical Neurosciences and by Novartis AG - both unrelated to this project. F. Paul has received honoraria and research support from Alexion, Bayer, Biogen, Chugai, MerckSerono, Novartis, Genyzme, MedImmune, Shire, and Teva Pharmaceuticals, and serves on scientific advisory boards for Alexion, MedImmune, Novartis, and UCB. He has received funding from Deutsche Forschungsgemeinschaft (DFG Exc 257), Bundesministerium für Bildung und Forschung (Competence Network Multiple Sclerosis), Guthy-Jackson Charitable Foundation, EU Framework Program 7, and National Multiple Sclerosis Society of the USA. He serves on the steering committee of the N-Momentum study with inebilizumab (Horizon Therapeutics) and the OCTiMS Study (Novartis). He is an associate editor with
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous