

A case of resected anaplastic carcinoma of the pancreas producing granulocyte-colony stimulating factor with literature review
- PMID: 39231851
- PMCID: PMC11374941
- DOI: 10.1186/s40792-024-02008-3
A case of resected anaplastic carcinoma of the pancreas producing granulocyte-colony stimulating factor with literature review
Abstract
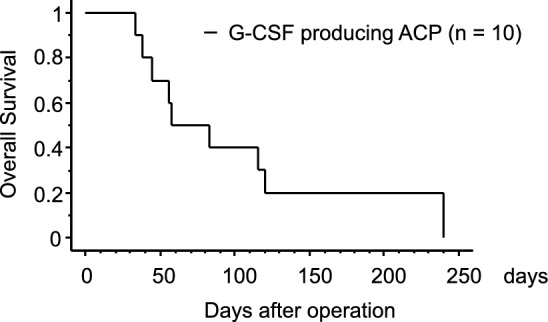
Background: Granulocyte colony-stimulating factor (G-CSF)-producing tumors have been reported in various organs, and the prognosis of patients with G-CSF-producing pancreatic cancers is particularly dismal. In this report, we present a case of G-CSF-producing anaplastic carcinoma of the pancreas (ACP), characterized by early postoperative recurrence and rapid, uncontrolled growth.
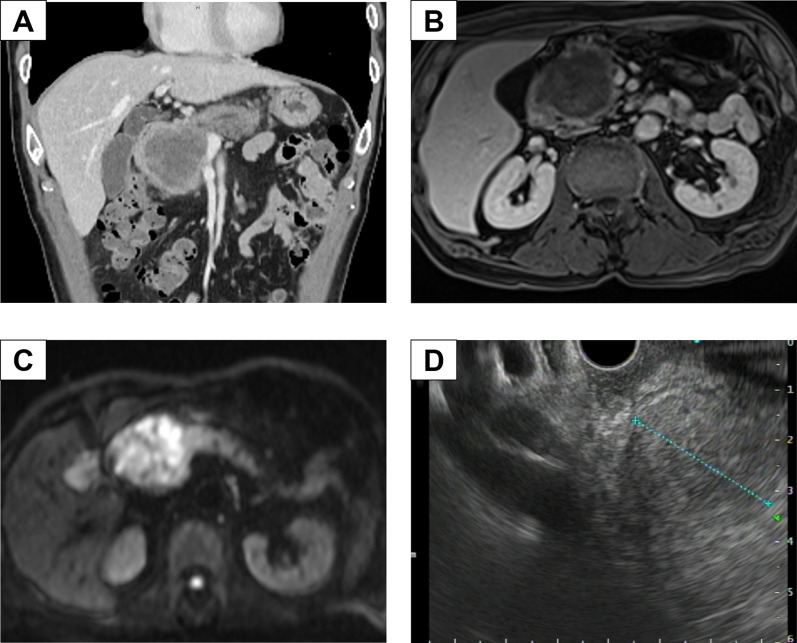
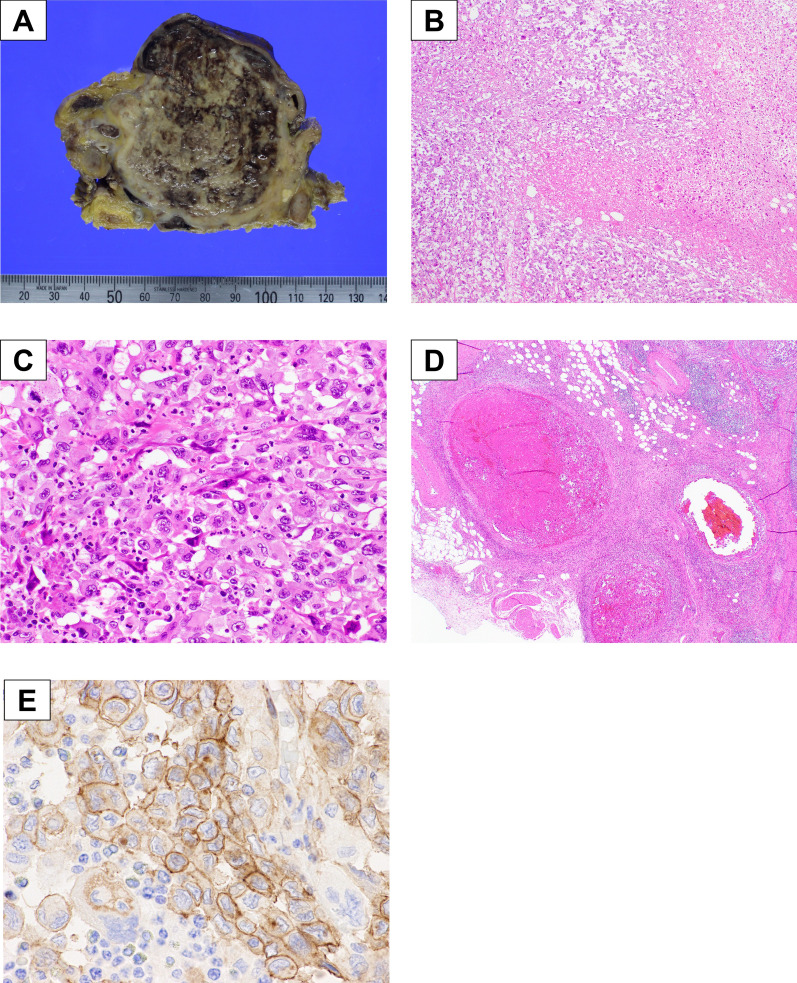
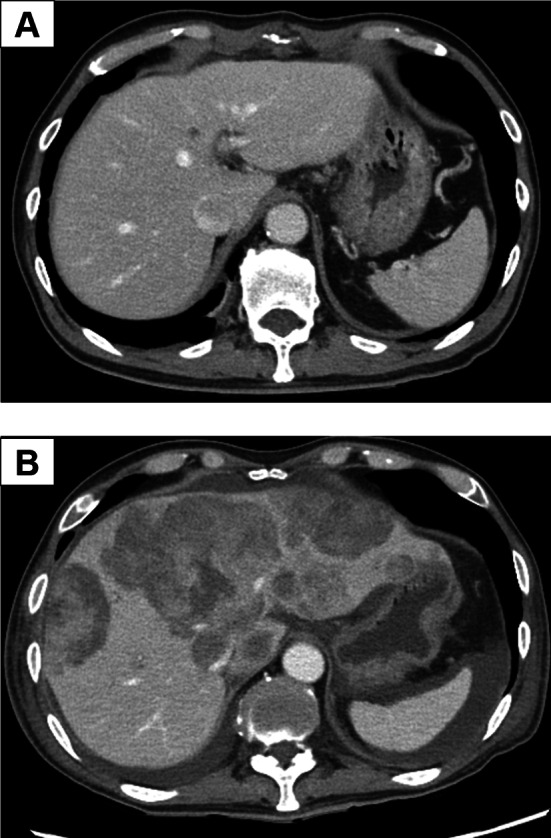
Case presentation: A 74-year-old man presented to our hospital with complaints of abdominal fullness and pain after eating. On admission, it was observed that the peripheral leukocyte counts and serum G-CSF levels were significantly elevated (23,770/µL and 251 pg/mL, respectively). Computed tomography of the abdomen revealed a pancreatic head tumor involving the superior mesenteric vein. Pathologically, ultrasound-guided fine-needle aspiration confirmed ACP. Subsequently, we performed a subtotal stomach-preserving pancreaticoduodenectomy with portal vein reconstruction and partial transverse colon resection. On postoperative day (POD) 7, the leukocyte count decreased from 21,180/μL to 8490/μL; moreover, computed tomography revealed liver metastasis. Therefore, mFOLFILINOX chemotherapy was initiated on POD 30. However, the tumor exhibited rapid progression, and the patient died on POD 45.
Conclusions: G-CSF-producing ACP is rare, and the prognosis of patients is extremely poor. Basic research is required to develop effective drugs against G-CSF-producing tumors, and large-scale studies using national databases are needed to develop multidisciplinary treatment methods.
Keywords: Anaplastic carcinoma; Granulocyte-colony stimulating factor; Pleomorphic-type; Undifferentiated carcinoma.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Anaplastic carcinoma of the pancreas producing granulocyte-colony stimulating factor: a case report.J Med Case Rep. 2008 Dec 17;2:391. doi: 10.1186/1752-1947-2-391. J Med Case Rep. 2008. PMID: 19091098 Free PMC article.
-
Granulocyte-colony stimulating factor producing anaplastic carcinoma of the pancreas treated by distal pancreatectomy and chemotherapy: report of a case.Surg Case Rep. 2015;1(1):46. doi: 10.1186/s40792-015-0048-y. Epub 2015 May 30. Surg Case Rep. 2015. PMID: 26366343 Free PMC article.
-
Granulocyte Colony-stimulating Factor Producing Anaplastic Carcinoma of the Pancreas: Case Report and Review of the Literature.Anticancer Res. 2017 Jan;37(1):223-228. doi: 10.21873/anticanres.11310. Anticancer Res. 2017. PMID: 28011495
-
[Resection of a Granulocyte Colony-Stimulating Factor-Producing Anaplastic Carcinoma of the Pancreas, Associated with Humoral Hypercalcemia of Malignancy].Gan To Kagaku Ryoho. 2018 May;45(5):859-862. Gan To Kagaku Ryoho. 2018. PMID: 30026452 Review. Japanese.
-
Granulocyte colony-stimulating factor-producing cutaneous squamous cell carcinoma: A case report and literature review.Medicine (Baltimore). 2025 Jun 6;104(23):e42798. doi: 10.1097/MD.0000000000042798. Medicine (Baltimore). 2025. PMID: 40489826 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
