

Artificial intelligence for ultrasonographic detection and diagnosis of hepatocellular carcinoma and cholangiocarcinoma
- PMID: 39232086
- PMCID: PMC11375009
- DOI: 10.1038/s41598-024-71657-z
Artificial intelligence for ultrasonographic detection and diagnosis of hepatocellular carcinoma and cholangiocarcinoma
Abstract
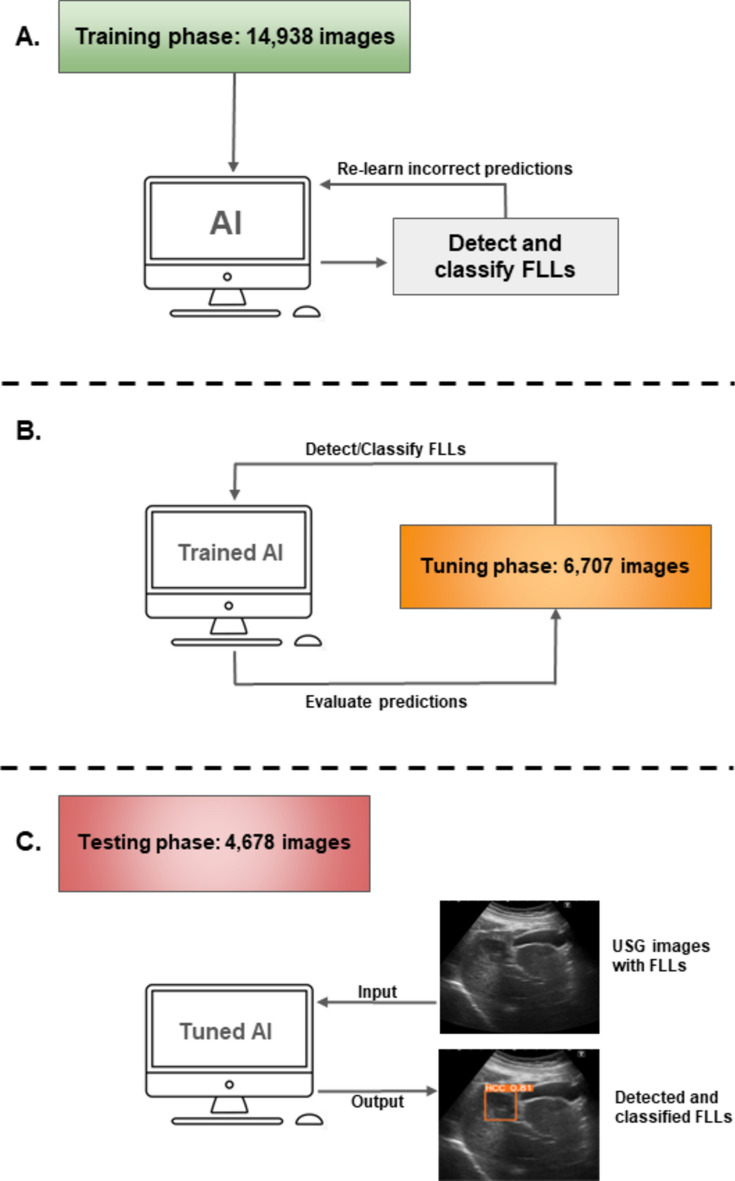
The effectiveness of ultrasonography (USG) in liver cancer screening is partly constrained by the operator's expertise. We aimed to develop and evaluate an AI-assisted system for detecting and classifying focal liver lesions (FLLs) from USG images. This retrospective study incorporated 26,288 USG images from 5444 patients to train YOLOv5 model for FLLs detection and classification of seven different types of FLLs, including hepatocellular carcinoma (HCC), cholangiocarcinoma (CCA), focal fatty infiltration, focal fatty sparing (FFS), cyst, hemangioma, and regenerative nodules. AI model performance was assessed for detection and diagnosis of the FLLs on a per-image and per-lesion basis. The AI achieved an overall FLLs detection rate of 84.8% (95%CI:83.3-86.4), with consistent performance for FLLs ≤ 1 cm and > 1 cm. It also exhibited sensitivity and specificity for distinguishing malignant FLLs from other benign FLLs at 97.0% (95%CI:95. 9-98.2) and 97.0% (95%CI:95.9-98.1), respectively. Among specific FLL types, CCA detection rate was at 92.2% (95%CI:88.0-96.4), followed by FFS at 89.7% (95%CI:87.1-92.3), and HCC at 82.3% (95%CI:77.1-87.5). The specificities and NPVs for regenerative nodules were 100% and 99.9% (95%CI:99.8-100.0), respectively. Our AI model can potentially assist physicians in FLLs detection and diagnosis during USG examinations. Further external validation is needed for clinical application.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
Grants and funding
- (NRCT): N42A640330/Digital Economy and Society Development Fund, Office of the National Digital Economy and Society Commission, Ministry of Digital Economy and Society, Thailand; National Research Council of Thailand
- (HEA663000011)/Thailand Science research and Innovation Fund Chulalongkorn University
- (HEA663000011)/Thailand Science research and Innovation Fund Chulalongkorn University
LinkOut - more resources
Full Text Sources
Medical
