

Artificial intelligence-assisted interventions for perioperative anesthetic management: a systematic review and meta-analysis
- PMID: 39232648
- PMCID: PMC11373311
- DOI: 10.1186/s12871-024-02699-z
Artificial intelligence-assisted interventions for perioperative anesthetic management: a systematic review and meta-analysis
Abstract
Background: Integration of artificial intelligence (AI) into medical practice has increased recently. Numerous AI models have been developed in the field of anesthesiology; however, their use in clinical settings remains limited. This study aimed to identify the gap between AI research and its implementation in anesthesiology via a systematic review of randomized controlled trials with meta-analysis (CRD42022353727).
Methods: We searched the databases of Medical Literature Analysis and Retrieval System Online (MEDLINE), Excerpta Medica Database (Embase), Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), Institute of Electrical and Electronics Engineers Xplore (IEEE), and Google Scholar and retrieved randomized controlled trials comparing conventional and AI-assisted anesthetic management published between the date of inception of the database and August 31, 2023.
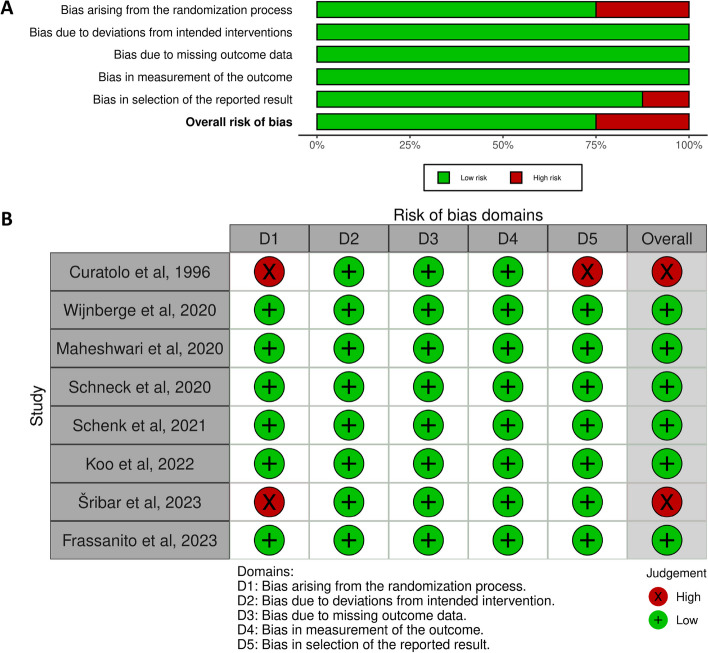
Results: Eight randomized controlled trials were included in this systematic review (n = 568 patients), including 286 and 282 patients who underwent anesthetic management with and without AI-assisted interventions, respectively. AI-assisted interventions used in the studies included fuzzy logic control for gas concentrations (one study) and the Hypotension Prediction Index (seven studies; adding only one indicator). Seven studies had small sample sizes (n = 30 to 68, except for the largest), and meta-analysis including the study with the largest sample size (n = 213) showed no difference in a hypotension-related outcome (mean difference of the time-weighted average of the area under the threshold 0.22, 95% confidence interval -0.03 to 0.48, P = 0.215, I2 93.8%).
Conclusions: This systematic review and meta-analysis revealed that randomized controlled trials on AI-assisted interventions in anesthesiology are in their infancy, and approaches that take into account complex clinical practice should be investigated in the future.
Trial registration: This study was registered with the International Prospective Register of Systematic Reviews (PROSPERO ID: CRD42022353727).
Keywords: Anesthesia; Artificial intelligence; Meta-analysis; Rondomized controlled trial; Systematic review.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Integration of Artificial Intelligence Into Sociotechnical Work Systems-Effects of Artificial Intelligence Solutions in Medical Imaging on Clinical Efficiency: Protocol for a Systematic Literature Review.JMIR Res Protoc. 2022 Dec 1;11(12):e40485. doi: 10.2196/40485. JMIR Res Protoc. 2022. PMID: 36454624 Free PMC article.
-
Artificial Intelligence (AI)-Driven Approaches to Manage Postoperative Pain, Anxiety, and Psychological Outcomes in Surgical Patients: A Systematic Review.Cureus. 2025 May 16;17(5):e84226. doi: 10.7759/cureus.84226. eCollection 2025 May. Cureus. 2025. PMID: 40519390 Free PMC article. Review.
-
Evaluation of Artificial Intelligence Algorithms for Diabetic Retinopathy Detection: Protocol for a Systematic Review and Meta-Analysis.JMIR Res Protoc. 2024 May 27;13:e57292. doi: 10.2196/57292. JMIR Res Protoc. 2024. PMID: 38801771 Free PMC article.
-
Interventions for adults with a history of complex traumatic events: the INCiTE mixed-methods systematic review.Health Technol Assess. 2020 Sep;24(43):1-312. doi: 10.3310/hta24430. Health Technol Assess. 2020. PMID: 32924926 Free PMC article.
References
-
- Xue B, Li D, Lu C, King CR, Wildes T, Avidan MS, Kannampallil T, Abraham J. Use of machine learning to develop and evaluate models using preoperative and intraoperative data to identify risks of postoperative complications. JAMA Netw Open. 2021;4(3):e212240. 10.1001/jamanetworkopen.2021.2240 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
