

Idiopathic intracranial hypertension in Asians: a retrospective dual-center study
- PMID: 39232671
- PMCID: PMC11373263
- DOI: 10.1186/s10194-024-01852-w
Idiopathic intracranial hypertension in Asians: a retrospective dual-center study
Abstract
Background: There have been limited data on idiopathic intracranial hypertension (IIH) in Asians and there remain uncertainties whether a cerebrospinal fluid (CSF) pressure of 250 mm CSF is an optimum diagnostic cutoff. The aims of the present study included (1) characterization of IIH patients in Taiwan, (2) comparisons among different diagnostic criteria for IIH, and (3) comparisons between patients with CSF pressures of > 250 and 200-250 mm CSF.
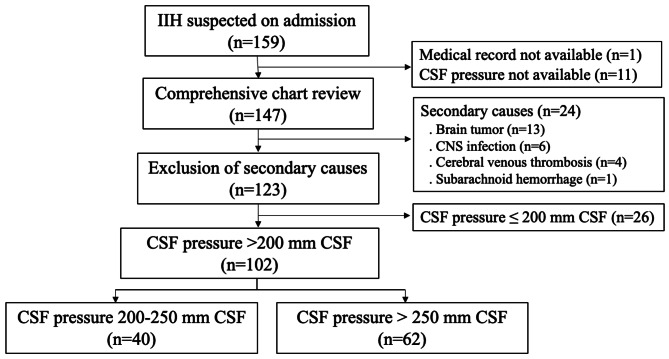
Methods: This retrospective study involved IIH patients based on the modified Dandy criteria from two tertiary medical centers in Taiwan. Clinical manifestations were retrieved from electronic medical records, and findings on ophthalmologic examination and magnetic resonance images (MRIs) were reviewed.
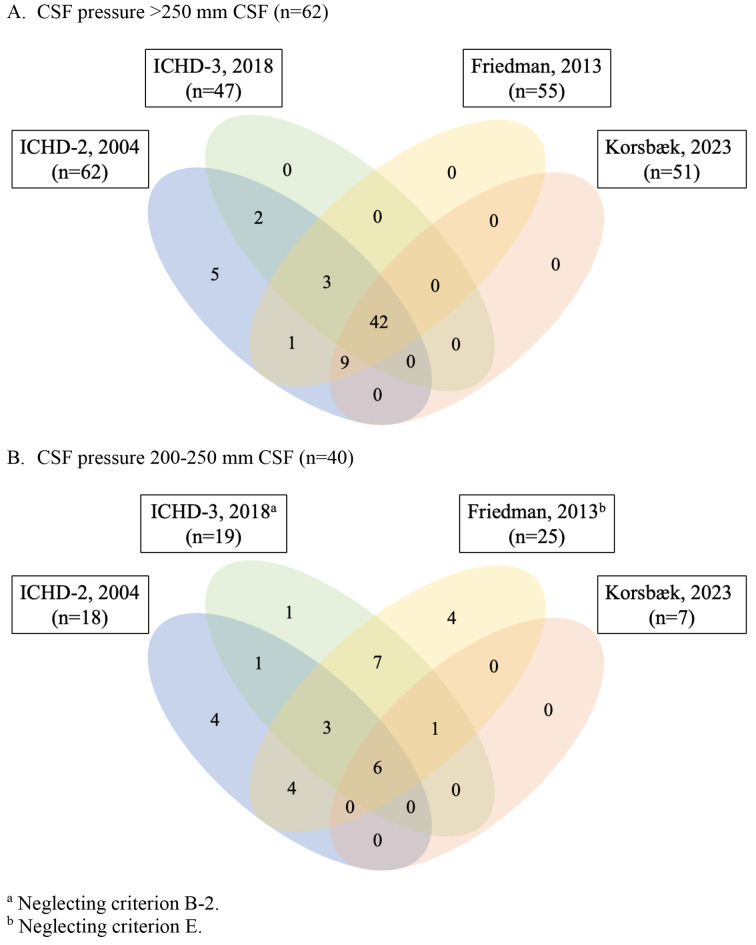
Results: A total of 102 patients (71 F/31 M, mean age 33.4 ± 12.2 years, mean CSF pressure 282.5 ± 74.5 mm CSF) were identified, including 46 (45.1%) with obesity (body-mass index ≥ 27.5), and 57 (62.6%) with papilledema. Overall, 80 (78.4%), 55 (53.9%), 51 (50.0%), and 58 (56.9%) patients met the Second and Third Edition of International Classification of Headache Disorders, Friedman, and Korsbæk criteria, respectively. Patients in the 200-250 mm CSF group (n = 40) were less likely to have papilledema (48.5% vs. 70.7%, p = 0.035), transient visual obscuration (12.5% vs. 33.9%, p = 0.005), and horizontal diplopia (10.0% vs. 30.6%, p = 0.006), and had fewer signs on MRIs (2.2 ± 1.3 vs. 2.8 ± 1.0, p = 0.021) when compared with those with CSF pressures > 250 mm CSF (n = 62). However, the percentages of patients with headache (95.0% vs. 87.1%, p = 0.109) at baseline, chronic migraine at six months (31.6% vs. 25.0%, p = 0.578), and visual field defect (86.7% vs. 90.3%, p = 0.709) were similar.
Conclusions: It was found that obesity and papilledema were less common in Asian IIH patients when compared with Caucasian patients. Although patients with CSF pressures of 200-250 mm CSF had a less severe phenotype, the risks of having headache or visual loss were comparable to those in the > 250 mm CSF group. It is possible that a diagnostic cutoff of > 200 mm CSF could be more suitable for Asians, although further studies are still needed.
Keywords: Criteria; Ethnicity; Idiopathic intracranial hypertension; Magnetic resonance imaging; Papilledema.
© 2024. The Author(s).
Conflict of interest statement
W.T.C. has received honoraria as a speaker from Allergan/AbbVie, Hava Bio-Pharma, Orient EuroPharma, Pfizer, and Viatris. He has received research grants from the Taiwan National Science and Technology Council, and Taipei Veterans General Hospital. S.J.W. has received personal fees as an advisor or speaker from AbbVie, Orient EuroPharma, Pfizer, and Percept; and has been the PI in trials sponsored by Allergan/AbbVie, Lundbeck, Novartis, Pfizer, and Orient EuroPharma. He has received research grants from the Taiwan National Science and Technology Council and Taipei Veterans General Hospital. Y.F.W. has received personal fees as an advisor or a speaker from Allergan/AbbVie, Boehringer Ingelheim, Chugai, Daiichi-Sankyo, Eli Lilly, Hava Bio-Pharma, Lundbeck, Novartis, Orient EuroPharma, Pfizer, Sanofi, Teva, UCB, and Viatris. He has received research grants from the Taiwan National Science and Technology Council, and Taipei Veterans General Hospital. H.T.H, H.C.C., T.W.H., Y.S.T., J.L.F., S.P.C., W.J.L., Y.W.P., Y.C.L., and J.F.L. reported no relevant disclosure.
Figures
References
Publication types
MeSH terms
Grants and funding
- 110-2321-B-010-005, 111-2321-B-A49-004, 111-2314-B-075 -086 -MY3, 111-2321-B-A49-011, and 112-2321-B-075-007/National Science and Technology Council
- 109-2314-B-075 -054 and 110-2314-B-075 -041 -MY3/National Science and Technology Council
- MOHW112-TDU-B-211-144001/Ministry of Health and Welfare
- V108C-092, V109C-096, V110C-111, V111C-161, V112C-078, V113C-123, and V112D67-003-MY3/Taipei Veterans General Hospital
LinkOut - more resources
Full Text Sources
Miscellaneous
